
Hemorrhoid pictures types symptoms are the three pillars of meaningful self-assessment: hemorrhoids present as either internal or external swollen vascular structures, each producing a recognizable symptom cluster that appears consistently in clinical photography. For those seeking a broader overview of related anorectal conditions, the hemorrhoid resource section covers management strategies, treatment comparisons, and condition guides. According to the National Institute of Diabetes and Digestive and Kidney Diseases, approximately 75% of adults will develop symptomatic hemorrhoids at some point — yet a substantial portion go unmanaged for months because the visual presentation is misread or attributed to other causes.
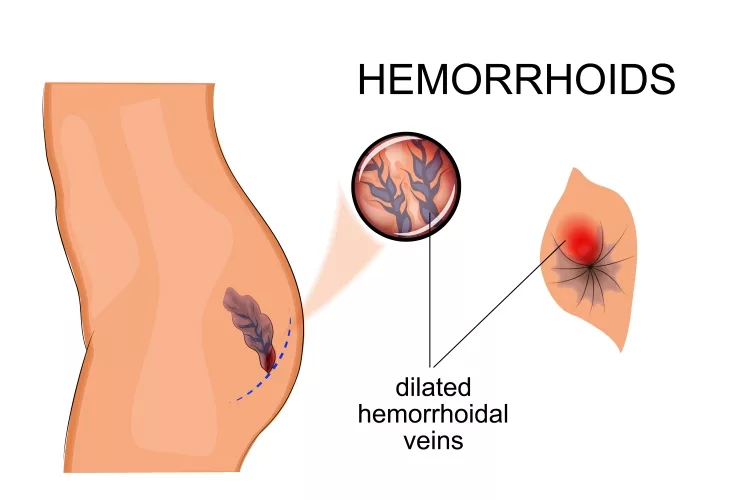
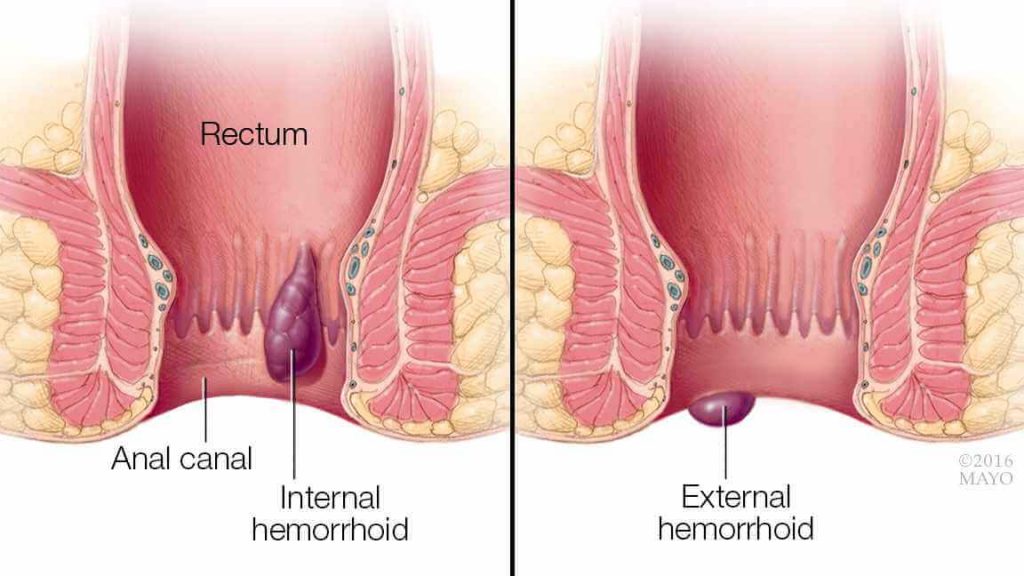
Hemorrhoids — clinically termed piles — are enlarged cushions of submucosal vascular tissue located in the anal canal and surrounding perianal region. Under normal anatomical conditions, these vascular cushions assist with stool continence and fine-tuned rectal control. When they become engorged, inflamed, or displaced, they transform into painful, bleeding lesions that drive millions of clinical visits each year. The distinction between types matters clinically: internal hemorrhoids arise above the dentate line and are typically painless in early grades, while external hemorrhoids develop below it and almost always produce discomfort, especially when thrombosed.
Chronic straining during bowel movements, a low-fiber diet, prolonged toilet sitting, and elevated intra-abdominal pressure — from obesity or pregnancy — are the most consistently identified risk factors in the literature. Recognizing the exact type and grade present determines whether conservative care resolves the issue or procedural intervention is warranted. This guide walks through every major classification, symptom pattern, staging system, and treatment pathway, supported throughout by clinical photographs and anatomical infographics.
Contents
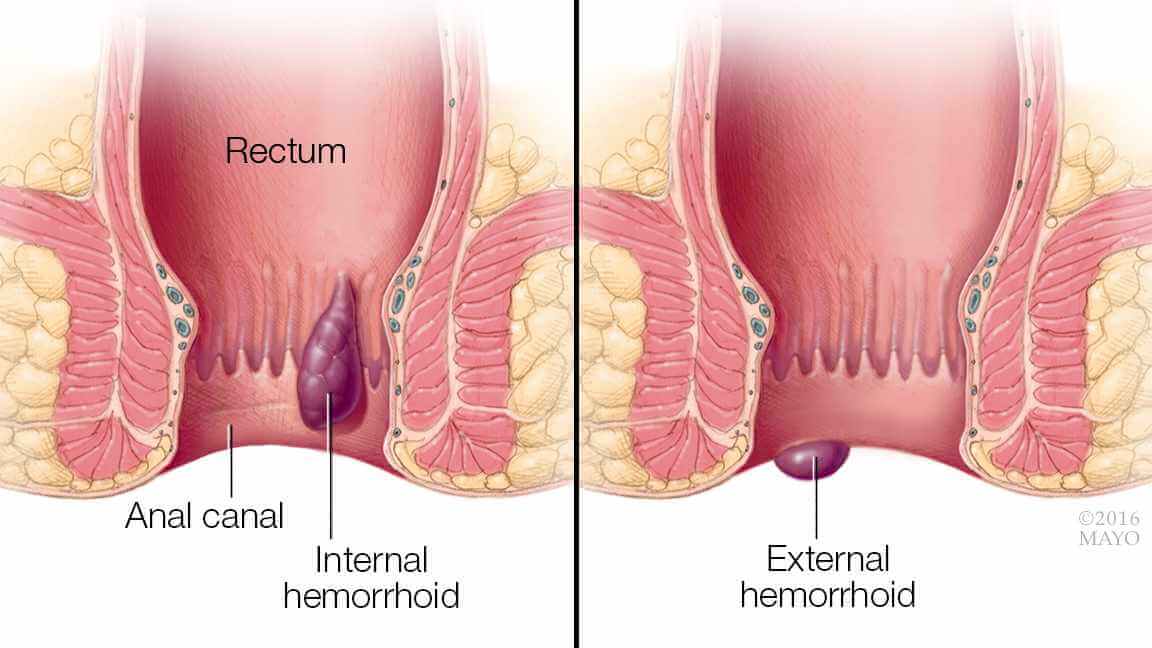
Clinical photographs of hemorrhoids serve a purpose beyond illustration — they establish diagnostic clarity for patients who cannot easily self-examine. The hemorrhoid pictures types symptoms framework begins with anatomical location. The dentate line — the internal boundary between columnar and squamous epithelium — is the definitive anatomical marker separating internal from external forms. Every classification decision flows from this single anatomical reference point.
Internal hemorrhoids develop within the anal canal, above the dentate line. Because this region lacks somatic pain receptors, internal hemorrhoids are classically painless — the hallmark symptom is bright red blood on toilet paper or pooling in the bowl after defecation, without accompanying discomfort. In clinical photographs, internal hemorrhoids appear as reddish, moist protrusions with smooth, glistening surfaces when prolapsed. They are graded on a four-point scale that directly governs treatment selection, discussed in detail in the staging section below.

External hemorrhoids form beneath the dentate line, within the perianal skin. This region is richly innervated by somatic pain fibers, which explains why external hemorrhoids produce significant discomfort — particularly when thrombosed. Visually, non-thrombosed external hemorrhoids appear as soft, flesh-toned bulges around the anal opening. Skin tags — fibrous remnants from previously thrombosed external hemorrhoids — are a common residual finding that patients frequently mistake for active disease. Distinguishing a skin tag from an active external hemorrhoid matters: skin tags require no treatment, while active thrombosed hemorrhoids may require urgent excision.


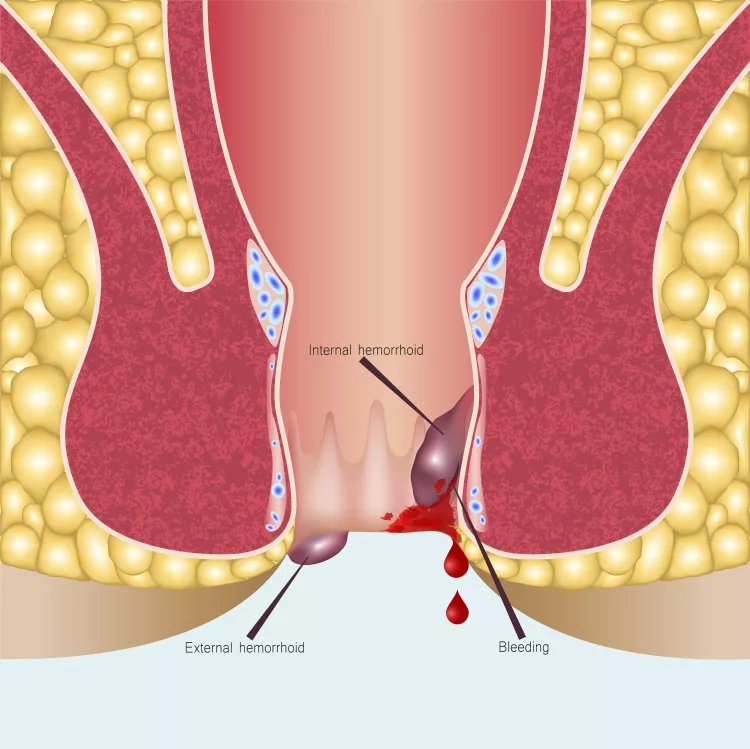
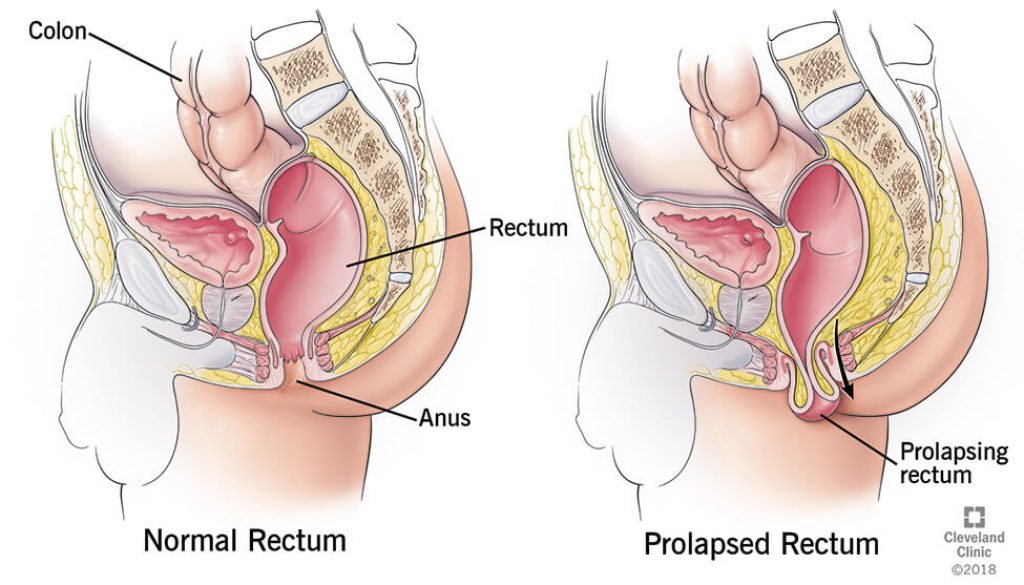
Prolapsed hemorrhoids occur when internal hemorrhoids descend through the anal canal and protrude externally. Prolapse progresses through grades III and IV of the standard classification. Thrombosed hemorrhoids — internal or external — contain a blood clot within the vascular tissue and represent an acute complication. They present as firm, acutely tender masses and produce pain that spikes dramatically with sitting, walking, or bowel movements. In photographs, thrombosed external hemorrhoids appear distinctly dark — purple to near-black — due to trapped, clotted blood beneath the overlying skin.


Clinical tip: A thrombosed external hemorrhoid presenting within 72 hours of onset is a strong candidate for office excision — waiting beyond this window makes the clot less accessible and significantly increases procedural complexity and patient discomfort.







Accurate symptom recognition is the foundation of safe self-management. Rectal bleeding should never be attributed to hemorrhoids without first ruling out other anorectal and colorectal pathology — colorectal cancer, inflammatory bowel disease, anal fissures, and rectal polyps can all produce overlapping presentations. The hemorrhoid pictures types symptoms distinction hinges on a careful assessment of bleeding character, pain location, tissue appearance, and associated sensations. For a similar visual-diagnostic approach applied to another inflammatory condition, the guide on gout pictures and infographics demonstrates how clinical photography clarifies what descriptive text alone cannot.
External hemorrhoids produce symptoms most patients identify immediately: pain or aching around the anus that worsens with sitting, defecation, or sustained physical activity. Itching — technically termed pruritus ani — is common, driven by perianal moisture, mucus leakage, and skin irritation from the hemorrhoidal tissue. Swelling is both visible and palpable. Bleeding from external hemorrhoids typically presents as bright red blood on toilet paper rather than dripping into the bowl — a pattern that differs meaningfully from the free-flowing rectal bleed associated with internal hemorrhoids or more proximal pathology.


Clinical photographs of external hemorrhoids reveal perianal skin with visible protrusions ranging from smooth, flesh-colored bumps to darker, engorged masses when thrombosis has occurred. Skin tags persist after resolution and are a reliable clinical sign of prior thrombotic episodes — their presence should prompt a thorough history to determine whether active hemorrhoidal disease remains.


Internal hemorrhoids are often completely asymptomatic in early grades. The first clinical sign is painless rectal bleeding — characteristically bright red, appearing after or during defecation. As the condition progresses, a sensation of incomplete evacuation or rectal fullness develops. Advanced internal hemorrhoids produce mucus discharge, perianal soiling, and persistent discomfort as prolapsed tissue rubs against perianal skin. The absence of acute pain in early-grade internal hemorrhoids is precisely why so many people delay evaluation — they assume that a painless bleed is trivial. It rarely is.

Hemorrhoids affect both sexes, though the triggers differ by population. Pregnancy creates sustained intra-abdominal pressure, making piles a near-universal complaint in the third trimester. Among males, the primary drivers are occupational sedentary behavior, chronic constipation, and habitual straining. Visual comparisons of piles presentations in females versus males in clinical photography reveal similar hemorrhoidal morphology but different distributions related to pelvic floor architecture and intra-abdominal pressure patterns.








Warning: Rectal bleeding that persists beyond two weeks, appears dark or maroon in color, or accompanies changes in bowel habits warrants immediate colorectal evaluation — these are not consistent with uncomplicated hemorrhoids and may indicate more serious pathology.
The grading system for internal hemorrhoids was developed to match treatment intensity to disease severity. Hemorrhoid pictures types symptoms correspond predictably to each grade, making visual references particularly valuable for both patients and clinicians navigating treatment decisions. Understanding that grade determines procedure removes ambiguity from the clinical pathway. For an analogous framework applied to another chronic inflammatory condition, the guide on arthritis and gout types, risks, and symptoms shows how structured grading systems streamline clinical decision-making across musculoskeletal and inflammatory diseases.
Grade I hemorrhoids are confined within the anal canal, do not prolapse, and are identified only through anoscopy or flexible endoscopy. The dominant symptom is intermittent painless bleeding after defecation. Grade II hemorrhoids prolapse during straining but reduce spontaneously — patients may notice a transient bulge that resolves without manual assistance.


Grade III hemorrhoids prolapse with straining and require manual reduction — patients must physically reposition the tissue back inside the anal canal. This grade marks the clinical boundary between office-based procedures and surgical consideration. Grade IV hemorrhoids are permanently prolapsed and cannot be manually reduced. Ulceration, incarceration, and strangulation are potential complications at this stage, all of which are visible in clinical photography as necrotic, darkened, or excoriated tissue surrounding the anal opening.





Grades I and II respond well to conservative management — dietary fiber supplementation, sitz baths, and topical corticosteroid or anesthetic preparations. Office-based procedures (rubber band ligation, infrared coagulation, sclerotherapy) are highly effective for grades II and III. Grade IV and complex grade III cases, along with most thrombosed external hemorrhoids that fail initial conservative management, require formal hemorrhoidectomy. Applying topical creams to a grade IV hemorrhoid is not only ineffective — it delays definitive care and allows complications to accumulate. Just as chronic conditions worsen without appropriate intervention — as detailed in the article on what happens when fibromyalgia is left untreated — hemorrhoids follow a predictable trajectory of deterioration when inadequately managed.
The financial landscape of hemorrhoid treatment ranges from under $30 per month to several thousand dollars, depending on severity and intervention type. Understanding the cost breakdown helps patients make informed decisions without unnecessary escalation or, conversely, without avoiding care due to cost assumptions. Insurance coverage varies substantially across plans and procedure codes, so direct verification with the payer is always the correct first step before scheduling any office procedure or surgery.
For grades I and II, conservative management is the standard first-line approach. Psyllium husk fiber supplements, osmotic stool softeners, warm sitz baths, and topical preparations containing hydrocortisone or lidocaine address the immediate symptom burden reliably. The total monthly outlay for a comprehensive conservative regimen rarely exceeds $40–$60. Consistent application over four to six weeks resolves the majority of early-grade hemorrhoids without clinical intervention. Evidence-based treatment protocols for pain conditions — similar to those outlined in the plantar fasciitis treatment framework — consistently demonstrate that addressing root causes (in this case, straining and constipation) produces better long-term outcomes than symptom management alone.
When conservative care fails or hemorrhoids reach grade III–IV, procedural intervention becomes necessary. Office-based procedures — performed without general anesthesia in a clinic setting — represent the middle tier of treatment intensity and cost. Surgical hemorrhoidectomy is reserved for refractory or severely prolapsed cases and carries the highest efficacy alongside the longest recovery period.
| Treatment Option | Estimated Cost (USD) | Setting | Recovery Time |
|---|---|---|---|
| OTC creams and suppositories | $5–$30 per month | Home | None |
| Sitz bath kit and fiber supplements | $15–$50 one-time | Home | None |
| Rubber band ligation (RBL) | $500–$1,500 per session | Outpatient clinic | 1–3 days |
| Infrared coagulation (IRC) | $400–$1,200 per session | Outpatient clinic | 1–2 days |
| Sclerotherapy | $300–$800 per session | Outpatient clinic | None to 1 day |
| Hemorrhoidectomy (surgical excision) | $3,000–$10,000 | Hospital or surgery center | 2–4 weeks |
| Stapled hemorrhoidopexy (PPH) | $2,500–$8,000 | Hospital or surgery center | 1–2 weeks |
Rubber band ligation remains the most widely performed office procedure for grade II–III internal hemorrhoids. A rubber band is placed at the base of the hemorrhoid, cutting off blood supply; the tissue necroses and sloughs within approximately one week. Infrared coagulation uses targeted heat to achieve hemostasis and works best on smaller grade I–II hemorrhoids. Laser surgery, while more expensive, produces less post-procedural pain and allows faster return to activity — an increasingly preferred option in specialized colorectal centers with appropriate equipment.




Treating an active hemorrhoid without addressing the underlying drivers guarantees recurrence. The long-term management framework for hemorrhoids is built on a small number of evidence-based interventions that, applied consistently, reduce symptomatic flares dramatically. Recurrence rates following conservative treatment alone run as high as 50% within five years — procedural and surgical outcomes are significantly better, but lifestyle modification remains the essential foundation regardless of intervention tier.
Dietary fiber is the single most impactful nutritional variable in hemorrhoid prevention. A target of 25–35 grams of fiber per day — from whole grains, legumes, vegetables, and fruit — normalizes stool consistency and eliminates the straining that drives vascular engorgement. Adequate fluid intake (eight to ten cups daily) works synergistically with fiber. Those exploring structured dietary changes to manage weight and reduce intra-abdominal pressure may find that approaches like the keto diet plan produce meaningful improvements, though fiber must be explicitly supplemented in any low-carbohydrate protocol to avoid constipation-driven straining.
Beyond diet, behavioral modification produces measurable results. Avoiding prolonged toilet sitting — ideally limiting time to under five minutes — removes one of the most consistent mechanical triggers. Regular physical activity improves gastrointestinal motility and reduces pelvic venous congestion. Obesity management directly lowers intra-abdominal pressure. For patients with occupational sedentary demands, standing breaks every 45–60 minutes represent a practical and effective intervention. Sitz baths taken after bowel movements reduce perianal inflammation during active flares and serve a preventive function between episodes when performed regularly.
Pro insight: Fiber supplements — psyllium in particular — are as effective as dietary fiber for hemorrhoid prevention, making supplementation a practical option for patients who cannot consistently meet whole-food fiber targets.
Hemorrhoids that recur more than twice per year despite consistent conservative management warrant formal colorectal evaluation. Persistent bleeding, new-onset change in stool caliber, unexplained weight loss, or a family history of colorectal cancer are all indications for colonoscopy alongside hemorrhoid management — not instead of it. Surveillance matters regardless of apparent hemorrhoid diagnosis. Clinicians who see patients self-managing with topical preparations for months without clinical assessment routinely identify conditions that would have been missed otherwise.
Post-procedural recurrence following rubber band ligation or infrared coagulation is common at three to five years and does not represent treatment failure — it represents disease chronicity that requires ongoing management. Repeat office procedures are appropriate and carry low cumulative risk. Surgical hemorrhoidectomy, when properly indicated, carries the lowest long-term recurrence rate of any available intervention and is frequently underutilized in patients who have tolerated years of symptomatic disease unnecessarily.
Hemorrhoid pictures types symptoms provide a reliable starting point for self-assessment, but clinical evaluation remains the only way to confirm grade, rule out competing pathology, and select the most appropriate treatment pathway. Anyone experiencing persistent rectal bleeding, prolapse, or pain unresponsive to two to four weeks of conservative care should schedule a colorectal consultation — and use the visual and clinical frameworks outlined here to arrive at that appointment with a clear, accurate account of what has been observed and for how long.





About Mehnaz
Mehnaz is the founder and editor of RipPain, a health resource site dedicated to helping readers navigate pain management, recovery, and medical device research. Her work on the site is driven by personal experience caring for seriously ill family members, which led her to study evidence-based guidance from physicians, pain specialists, and published medical research. She curates and summarizes expert medical insights to make credible health information accessible to everyday readers.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below