
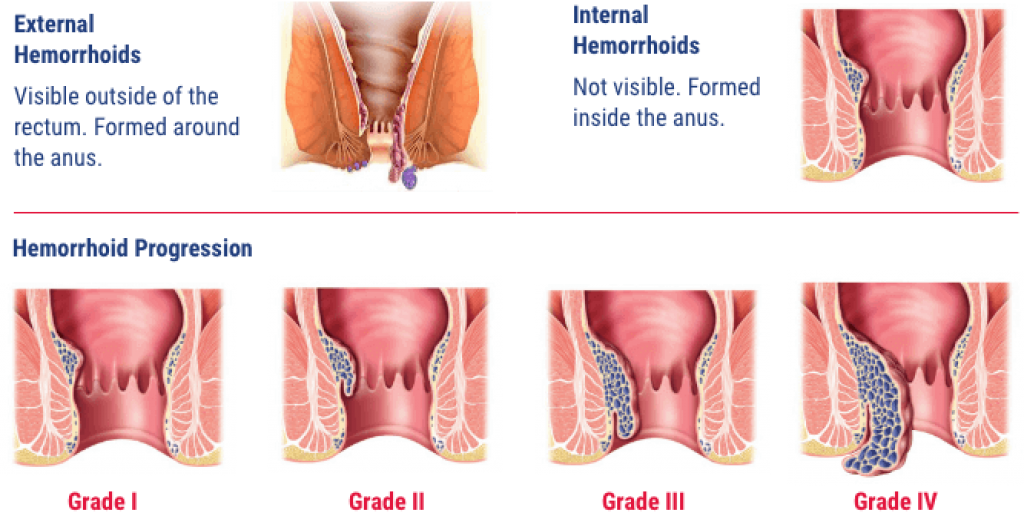
Hemorrhoid complications and risks are more serious than most people expect — and they escalate faster when left unmanaged. What starts as intermittent itching and discomfort can progress into rectal bleeding disorders, abscess formation, strangulation, and even a life-threatening delay in diagnosing colorectal cancer. If you're navigating this condition, start with a solid understanding of what hemorrhoids are and how they develop before tackling everything that can go wrong.
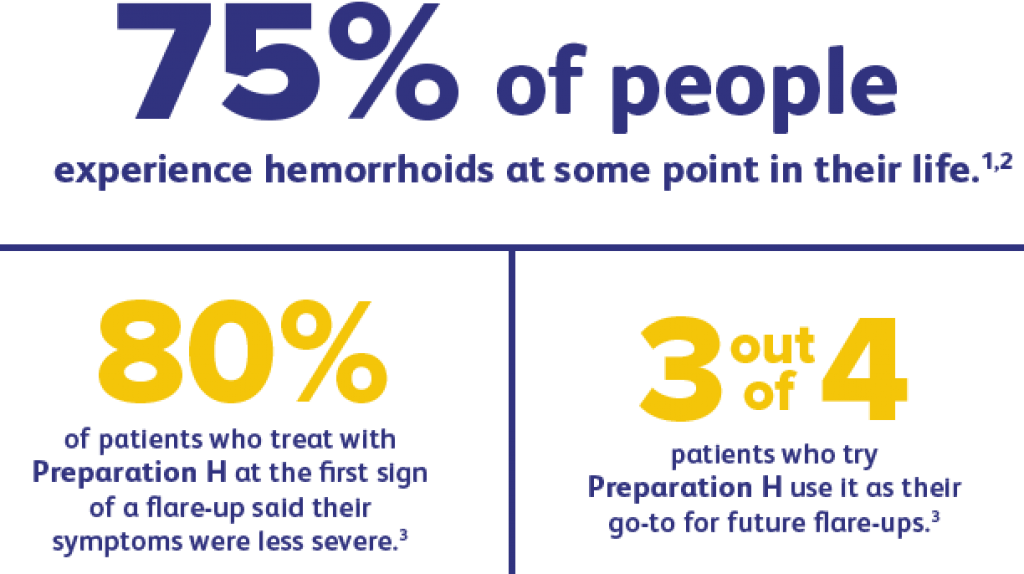
More than 75% of people will experience hemorrhoids at some point. They're the most common anorectal condition in the Western world — yet the majority of people either ignore symptoms until complications develop or treat them incorrectly and make things worse. Both paths lead to the same place: a preventable problem becoming a serious one.
This guide covers all 12 serious complications, the warning signs that signal escalation, the mistakes that accelerate damage, and the evidence-based strategies that give you real long-term protection. Whether you're managing an active case or trying to prevent a recurrence, this is what you need to know.
Contents
Not every complication carries the same urgency. Some cause significant localized pain; others create systemic health problems you won't immediately connect to your hemorrhoids. Here's the complete breakdown of what you're up against:
| # | Complication | Severity | Most Common In |
|---|---|---|---|
| 1 | Thrombosis (blood clot formation) | Moderate–Severe | External hemorrhoids |
| 2 | Severe rectal bleeding | Moderate–Severe | Internal Grade 3–4 |
| 3 | Iron-deficiency anemia | Moderate–Severe | Chronic, untreated cases |
| 4 | Strangulation | Severe | Prolapsed internal hemorrhoids |
| 5 | Perianal abscess or infection | Severe | Post-thrombosis, immunocompromised |
| 6 | Fistula formation | Moderate–Severe | Recurrent abscess |
| 7 | Anal fissures | Mild–Moderate | External and chronic hemorrhoids |
| 8 | Fecal incontinence | Severe | Grade 4, post-surgical |
| 9 | Progressive prolapse | Moderate–Severe | All internal grades |
| 10 | Perianal skin tags | Mild | Resolved external hemorrhoids |
| 11 | Gangrene (rare) | Life-threatening | Strangulated, immunocompromised |
| 12 | Masked colorectal cancer diagnosis | Life-threatening | Any age, any grade |
The most frequently encountered are rectal bleeding and thrombosis — but the most dangerous are anemia from chronic blood loss, infection, strangulation, and the critical error of assuming rectal bleeding is "just hemorrhoids" when cancer is the actual culprit.
Certain factors push your hemorrhoid complications and risks well above the population baseline:
Most hemorrhoid complications don't arrive without warning. Your body signals the escalation well before it becomes an emergency. These are the red flags that demand attention:
Use this structured process to gauge where you stand:
If multiple items on this list apply to you right now, don't sit with it. The longer a Grade 3 or Grade 4 hemorrhoid goes without treatment, the more permanent tissue damage accumulates — and the more likely you are to end up facing surgical intervention rather than an office procedure.
The single greatest driver of serious complications is delay. People wait weeks, months, or years before seeking help — often out of embarrassment or the belief that it will resolve on its own. Here's the real cost of that delay:
According to the National Institutes of Health, rectal bleeding should always be evaluated by a physician regardless of a known hemorrhoid diagnosis. Never assume bleeding is exclusively hemorrhoidal without a physician's confirmation.
Not every over-the-counter solution is safe or appropriate for every stage of hemorrhoids. These are the treatment errors that consistently worsen outcomes:

Fiber intake and hydration are your two most powerful preventive tools. The evidence on this is consistent across decades of research. Build your diet around these principles:
Regular low-impact exercise plays a critical role in both prevention and management. Sustained cardiovascular activity stimulates bowel motility and reduces constipation without placing mechanical pressure on the pelvic floor. Recumbent exercise bikes deliver outstanding benefits for people managing anorectal conditions because the reclined position eliminates most pelvic pressure during workouts. If you're looking for a specific recommendation, a quality recumbent bike for home cardio is one of the most practical investments you can make for long-term hemorrhoid management. For people with concurrent conditions like lower back pain, this same low-impact approach protects the lumbar spine while keeping you active.
Warning: Never sit on the toilet for more than 5 minutes. Every extra minute spent reading or scrolling while seated increases pelvic venous pressure and directly accelerates hemorrhoid progression.
What you do in the bathroom matters as much as your diet. These corrective steps interrupt the mechanical cycle that drives escalation:
The right topical product reduces inflammation, protects damaged tissue, and prevents secondary complications. These are the most clinically relevant categories and how to use them correctly:
| Product Type | Primary Benefit | Best For | Key Caution |
|---|---|---|---|
| Hydrocortisone cream (0.5–1%) | Reduces inflammation and itching | Short-term flare management | Do not use longer than 7 consecutive days |
| Witch hazel pads | Astringent — reduces swelling and soothes | External hemorrhoids, post-bowel hygiene | Avoid on broken or raw skin |
| Lidocaine topical gel | Local anesthetic for acute pain relief | Thrombosed external hemorrhoids | Temporary symptom control only |
| Zinc oxide ointment | Protective barrier, moisture control | Skin irritation, discharge-related breakdown | Low risk — safe for extended use |
| Natural / herbal balms | Gentle anti-inflammatory, skin soothing | Pregnancy-related hemorrhoids | Verify ingredient safety if pregnant |
| Rectal suppositories | Deliver medication to internal tissue | Internal Grade 1–2 hemorrhoids | Use exactly as directed — misuse increases irritation |
Several over-the-counter options have strong user track records for managing active symptoms. The products below represent commonly used hemorrhoid relief preparations:






A warm sitz bath — soaking the perianal area in 3–4 inches of warm (not hot) water for 15–20 minutes — is one of the most consistently effective evidence-backed methods for reducing inflammation and pain during a flare. Aim for 2–3 sessions per day during acute episodes.
For comprehensive information on the full hemorrhoid treatment landscape, including natural remedies, medical procedures, and prevention protocols, the category page covers every angle in detail.
Home management works reliably for Grade 1 and most Grade 2 hemorrhoids. These situations require a physician's assessment — promptly:

When home management isn't enough, several minimally invasive office procedures resolve Grade 2–3 internal hemorrhoids effectively:
Recovery from hemorrhoidectomy takes 2–4 weeks. Stool softeners, sitz baths, and appropriate analgesics are the pillars of postoperative management. Don't defer surgical consultation if you're at Grade 3 or 4. Every month of delay allows additional tissue damage to accumulate — making the eventual procedure harder and recovery longer. For people managing multiple pain conditions during recovery, understanding how to approach concurrent lower back pain is worth reviewing, since straining and altered posture during recovery can affect the lumbar region simultaneously.
Yes. While most cases are manageable, untreated hemorrhoids can lead to iron-deficiency anemia, perianal abscess, fistula, strangulation, and in rare cases gangrene. The most underappreciated risk is that hemorrhoid symptoms can mask a colorectal cancer diagnosis for months or years.
Grade 1 and Grade 2 hemorrhoids that receive no treatment or lifestyle modification typically progress. Chronic bleeding causes anemia. Repeated prolapse weakens the sphincter muscles over time, increasing the risk of fecal incontinence. Skin breakdown and recurring infections become increasingly common.
A thrombosed external hemorrhoid presents as a sudden, hard, extremely tender blue or purple lump at the anal opening. The pain is typically severe and constant rather than intermittent. It appears quickly — often within hours — and differs from the dull aching of a standard external hemorrhoid.
Yes. Chronic low-volume bleeding from internal hemorrhoids, even if it seems minor, can deplete iron stores over months. The result is iron-deficiency anemia with symptoms including persistent fatigue, pale skin, shortness of breath on exertion, and rapid heartbeat. Blood tests will confirm the diagnosis.
No — and this is critical. Rectal bleeding can originate from hemorrhoids, anal fissures, polyps, inflammatory bowel disease, or colorectal cancer. Any rectal bleeding warrants medical evaluation to confirm the source, especially in patients over 50 or those with a family history of colorectal cancer.
See a doctor if bleeding persists beyond one week, a prolapsed hemorrhoid won't reduce manually, you develop fever with rectal pain, or symptoms don't improve after two weeks of consistent home treatment. Don't wait for a complication to force the issue — early-stage hemorrhoids are far easier and less painful to treat.
Yes. Grade 4 prolapsed internal hemorrhoids that press chronically against the anal sphincter can impair its resting tone. Additionally, surgical treatments for advanced hemorrhoids carry a small but real risk of sphincter damage. This is one of the most compelling reasons to treat hemorrhoids before they reach Grade 4.
Hemorrhoids rarely become dangerous overnight — they become dangerous because the warning signs were ignored, one day at a time.





About Dr. Zhifei Sun, MD
Dr. Zhifei Sun is a colon and rectal surgeon affiliated with MedStar Georgetown University Hospital in Washington, D.C. He specializes in minimally invasive surgical techniques for colorectal diseases, including diverticular disease, ulcerative colitis, Crohn's disease, and colorectal cancer. His clinical work focuses on improving patient outcomes through laparoscopic and robotic-assisted approaches to complex colorectal conditions.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below