
The factors affecting pulse oximetry readings are more numerous — and more consequential — than most people realize. A pulse oximeter might display 97% SpO2 while the actual arterial saturation sits several points lower. Knowing what distorts these readings helps patients, caregivers, and clinicians make better decisions rather than acting on numbers that may be quietly misleading. For anyone monitoring oxygen saturation during a respiratory illness — such as those assessed in how to tell if bronchitis is turning into pneumonia — understanding these limitations is not optional. It is essential.

Pulse oximeters work by shining light through the skin to estimate blood oxygen saturation. The device is non-invasive, fast, and widely available — qualities that have made it a staple in emergency rooms, home health kits, and fitness tracking. But the technology carries real blind spots that can produce readings that are too high, too low, or simply unstable.
Anyone managing chronic respiratory issues, circulatory conditions, or anemia should understand when to trust the number on the screen and when to demand a more reliable measurement. This guide breaks down the science, the common pitfalls, and the practical protocols that produce readings which actually reflect what is happening inside the body.
Contents
A pulse oximeter clips onto a fingertip, earlobe, or toe and emits two wavelengths of light — red (660 nm) and infrared (940 nm). Oxygenated hemoglobin absorbs more infrared light, while deoxygenated hemoglobin absorbs more red light. The device calculates the ratio between these two absorption patterns and converts the result into a SpO2 percentage. This process happens continuously, producing a real-time estimate of blood oxygen saturation.
The key word is estimate. Pulse oximetry is not a direct measurement of arterial oxygen — it is an optical inference based on light absorption in peripheral tissue. That distinction matters enormously when the tissue is cold, poorly perfused, or covered by pigment-blocking material. For regulatory context on the clinical standards these devices must meet, the U.S. Food and Drug Administration's guidance on pulse oximeters explains why consumer devices differ significantly from clinical ones.
A healthy adult typically shows SpO2 values between 95% and 100%. Below 90% is considered hypoxemic and warrants immediate medical attention. Values between 90% and 94% are borderline and require clinical evaluation. These thresholds assume the device is measuring accurately — which, as this article makes clear, is not always the case.
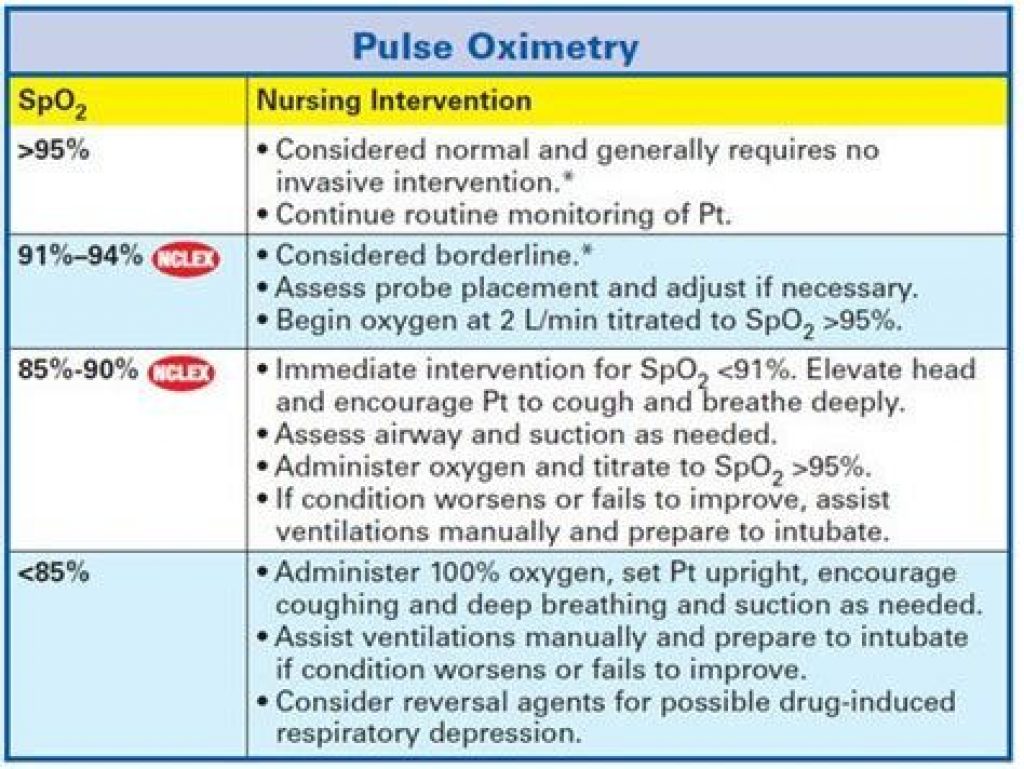
Understanding these reference ranges is the foundation for interpreting any reading correctly. It is equally important to recognize that the device producing those numbers may be generating false confidence — or unnecessary alarm — depending on conditions at the time of measurement.
The factors affecting pulse oximetry readings that originate inside the body are often the hardest to control. Several physiological conditions introduce systematic error into SpO2 values:
External conditions and the device itself introduce another layer of variability. These factors are generally more controllable than physiological ones, which makes addressing them a priority before attributing a reading to clinical change:
Motion artifact is the single most common cause of unreliable pulse oximetry readings in both clinical and home settings. When a patient moves — even subtly — the device registers fluctuating light absorption that it interprets as a pulsatile signal. The result is an erratic waveform and an SpO2 reading that may swing dramatically across a 10–20 second window.
Resolving motion artifact starts with patient positioning. The monitored hand should rest flat, ideally below heart level, with the probe seated firmly on the fingertip. If readings remain unstable, switching to the earlobe or a forehead reflectance probe often yields better results in high-motion scenarios such as dyspnea or involuntary tremor.
Pro tip: If a reading fluctuates by more than 3–4 percentage points over 10 seconds, the waveform is unreliable — wait for the signal to stabilize fully before recording the value.
Probe placement errors are equally problematic. The LED and photodetector must sit directly opposite each other across the finger. Misalignment — even slight rotation — reduces signal strength. Edematous fingers create excessive tissue depth between LED and detector, further attenuating the signal and producing artificially low readings that may prompt unnecessary intervention.
The relationship between skin tone and pulse oximetry accuracy has received significant scientific scrutiny. Studies published in peer-reviewed journals found that pulse oximeters overestimated SpO2 by 3–4% on average in patients with darker skin tones compared to those with lighter skin — a margin that can determine whether a patient receives timely treatment or is sent home with false reassurance.
Nail polish presents a more controllable problem. Dark polishes — blue, purple, green, and black — absorb red light wavelengths and artificially suppress readings. The standard fix is to rotate the probe 90 degrees so light transmits through the lateral aspects of the finger rather than through the nail bed. Removing polish from one finger before monitoring remains the most reliable solution. Acrylic and gel nails add another layer of material that reduces transmission quality; in these cases, the earlobe is a better probe site.
Accurate pulse oximetry starts before the clip goes on. A short preparation sequence dramatically reduces artifact-driven or physiologically distorted readings:
A consistent protocol each time produces more comparable and trustworthy data over time. This sequence applies to both clinical and home monitoring contexts:
Pulse oximetry performs well under specific conditions. Clinicians and home users can place greater confidence in readings when the following criteria are met:
Under these ideal conditions, a quality pulse oximeter tracks true arterial oxygen saturation within ±2%. That accuracy is sufficient for routine monitoring of patients with stable respiratory or cardiac conditions. Those tracking ongoing respiratory illness — including those evaluating whether coronavirus protection measures are effective for at-home triage — rely on this level of accuracy to make meaningful management decisions.
There are clear situations where pulse oximetry alone is not sufficient. In these cases, additional diagnostic tools are not optional — they are clinically necessary:
Patients managing severe respiratory conditions — including those wondering whether untreated bronchitis can become fatal — should understand that a reassuring pulse oximetry reading during a high-risk illness may not reflect the full clinical picture without confirmatory testing.
Not all pulse oximeters are equal. The device category matters as much as the measurement technique. Consumer units and clinical devices differ across every dimension that affects reliability:
| Feature | Consumer-Grade Oximeter | Hospital-Grade Oximeter |
|---|---|---|
| Accuracy range | ±3–5% (manufacturer-claimed) | ±2% (clinically validated) |
| Motion artifact handling | Basic signal averaging | Advanced processing (e.g., Masimo SET) |
| Low perfusion performance | Fails below perfusion index 0.4 | Functional down to perfusion index 0.02 |
| Alarm capability | Minimal or absent | Customizable SpO2 and heart rate alarms |
| Skin tone calibration | Rarely addressed | Newer models include multi-ethnic calibration |
| Regulatory clearance | Variable; may lack FDA 510(k) clearance | FDA 510(k) cleared with clinical trial data |
| Typical cost | $15–$80 | $200–$3,000+ |
For home use, an FDA-cleared device from a recognized manufacturer — Nonin, Masimo, or Contec — offers meaningfully better accuracy than generic alternatives. The medical instrument category on RipPain covers a range of validated monitoring tools suited to home health management across various chronic conditions.
Arterial blood gas analysis is the gold standard for assessing oxygenation, ventilation, and acid-base status. Unlike pulse oximetry, ABG provides direct measurement of PaO2 (partial pressure of arterial oxygen), hemoglobin saturation, CO2 levels, and blood pH — producing a complete metabolic picture that no fingertip device can replicate.
ABG requires an arterial puncture, trained staff, and laboratory processing. It is not a bedside screening tool. Pulse oximetry fills that role as a continuous, non-invasive surveillance method. The appropriate clinical model is to use pulse oximetry for ongoing monitoring and reserve ABG for diagnostic confirmation when results are unexpected, when clinical severity demands certainty, or when a known confounding factor makes SpO2 values inherently unreliable.
Clinicians who treat pulse oximetry as a definitive diagnostic tool — rather than a screening proxy — expose patients to the risk of both under-treatment and over-treatment. The technology is powerful precisely because it is understood for what it is: a real-time estimate, not a laboratory measurement.
The most common factors include motion artifacts, poor peripheral circulation, nail polish (especially dark colors), skin pigmentation, carbon monoxide poisoning, and anemia. Environmental issues such as bright ambient light and improperly sized probes also contribute to inaccurate results in both home and clinical settings.
Yes. Peer-reviewed research has confirmed that pulse oximeters consistently overestimate oxygen saturation in individuals with darker skin tones by an average of 3–4 percentage points. The overestimation occurs because device calibration algorithms do not adequately account for how melanin interacts with the red and infrared light wavelengths used in measurement.
Not always. Light-colored or sheer polishes have minimal impact on readings. Dark polishes — particularly black, blue, and green — do interfere with the red light wavelength and can suppress recorded SpO2. Rotating the probe 90 degrees to transmit through the lateral finger skin, or measuring at the earlobe, eliminates this source of error entirely.
A reading below 95% warrants attention, particularly if it persists across multiple stable measurements under controlled conditions. Readings below 90% indicate potential hypoxemia and require immediate clinical evaluation. Any reading that conflicts with the patient's visible symptoms — such as a high SpO2 in someone who is visibly short of breath — should prompt further diagnostic testing rather than reassurance based on the oximeter alone.
No. Standard two-wavelength pulse oximeters cannot distinguish between oxyhemoglobin and carboxyhemoglobin. In carbon monoxide poisoning, the device reports a falsely elevated SpO2 while the patient is actually severely hypoxic at the cellular level. Only a specialized co-oximeter or arterial blood gas analysis with co-oximetry can identify and quantify CO toxicity accurately.
Consumer-grade pulse oximeters are useful for trending data in stable patients but should not substitute for clinical-grade devices in high-stakes monitoring. For routine home use in otherwise healthy individuals or those with stable conditions, an FDA-cleared device from a reputable manufacturer is adequate. For patients with complex cardiovascular or respiratory disease, hospital-grade accuracy and validated signal processing are significantly more reliable.





About Mehnaz
Mehnaz is the founder and editor of RipPain, a health resource site dedicated to helping readers navigate pain management, recovery, and medical device research. Her work on the site is driven by personal experience caring for seriously ill family members, which led her to study evidence-based guidance from physicians, pain specialists, and published medical research. She curates and summarizes expert medical insights to make credible health information accessible to everyday readers.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below