
Can you die from bronchitis? Yes — in high-risk individuals and when left entirely without treatment, bronchitis can escalate into life-threatening respiratory failure. The comprehensive picture of bronchitis shows that while most healthy adults recover fully, specific populations face a very different clinical trajectory when symptoms are dismissed or managed incorrectly.
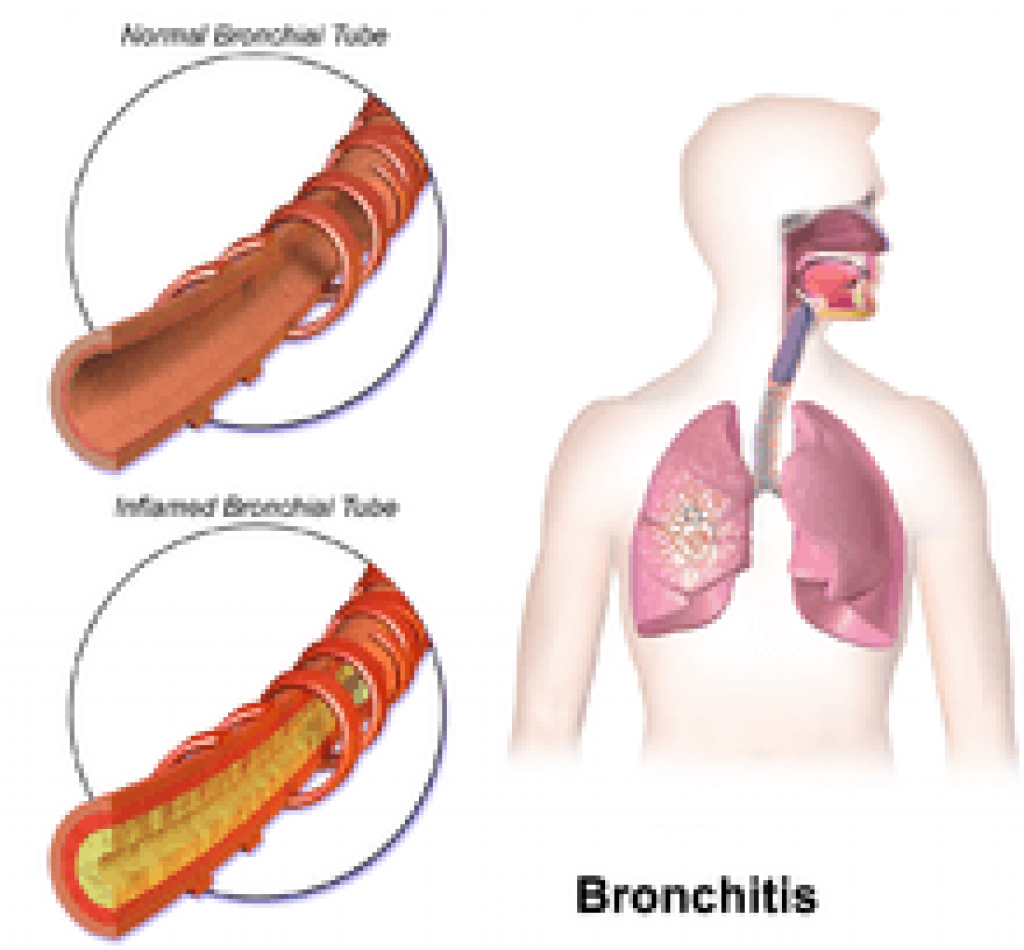
Bronchitis is inflammation of the bronchial tubes — the airways that carry oxygen to and from the lungs. It presents in two distinct clinical forms: acute bronchitis, typically triggered by viral pathogens and resolving within two to three weeks in healthy patients, and chronic bronchitis, a persistent condition defined by productive cough lasting at least three months over two consecutive years. Each form carries its own progression risk, and each can compound underlying health vulnerabilities in ways that turn a manageable illness into a genuine emergency.
The clinical record is consistent — patients who delay seeking evaluation for worsening respiratory symptoms face significantly elevated complication rates. A chest infection that begins as irritating bronchial inflammation can degrade into bacterial pneumonia, severe oxygen depletion, or systemic sepsis within days in vulnerable patients. Recognizing the escalation trajectory early is not about anxiety management — it is a fundamental survival consideration that every patient with chronic or recurrent respiratory illness should internalize.
Contents
The escalation pathway from routine bronchitis to fatal outcome is well-documented in pulmonary medicine, but it is rarely linear. Healthy adults with intact immune systems typically recover from acute bronchitis without prescription intervention beyond rest and hydration. The danger zone emerges when inflammation persists beyond three weeks, when secondary bacterial infection colonizes the already-damaged airways, or when the patient's baseline cardiopulmonary reserve cannot absorb the additional respiratory burden imposed by progressive disease.
Clinicians watch for a specific cluster of deteriorating symptoms that indicate bronchitis has moved beyond its benign phase. Cyanosis — a bluish discoloration around the lips or fingernails — signals severe oxygen deprivation and constitutes an emergency without exception. High fever persisting beyond three days, blood-streaked sputum, and chest pain that intensifies with each breath are equally non-negotiable indicators for immediate evaluation. Tracking blood oxygen with a quality pulse oximeter provides real-time data on saturation levels and can catch dangerous drops before they become visually apparent — a particularly important safeguard for patients managing bronchitis at home.
Adults over 65, infants under two years, and individuals with COPD, asthma, congestive heart failure, or diabetes face disproportionately severe outcomes when bronchitis goes unmanaged. Smokers constitute a particularly vulnerable subgroup — their airways are already compromised, ciliary function is suppressed, and inflammatory baseline is chronically elevated, creating conditions where acute exacerbations escalate with alarming speed. Immunocompromised patients receiving corticosteroids or chemotherapy face similarly compressed timelines, and any respiratory infection in these populations warrants prompt clinical assessment rather than watchful waiting.
Not all bronchitis carries equal mortality risk, and conflating the two forms leads patients to underestimate one while mismanaging the other. Acute and chronic bronchitis share a name but differ substantially in mechanism, duration, and long-term consequence for lung architecture.
Acute bronchitis typically follows an upper respiratory viral infection by three to four days. The bronchial lining becomes inflamed, mucus production surges, and the characteristic productive cough begins. In 85 to 95 percent of cases, the viral etiology means antibiotics offer no measurable benefit. The illness resolves within ten to twenty-one days in healthy adults, but failure to rest, maintain hydration, and manage fever adequately extends this window considerably and creates the conditions for secondary bacterial pneumonia to establish itself in the already-inflamed tissue.
Chronic bronchitis, one of the two primary diagnoses under the COPD umbrella, represents a fundamentally different clinical picture from its acute counterpart. The airway walls have undergone structural remodeling — mucus glands are hypertrophied, ciliary function is measurably compromised, and airflow obstruction is progressive. Each acute exacerbation accelerates this decline. Patients with advanced chronic bronchitis experience forced expiratory volumes that can drop below 50 percent of predicted values, and those patients face genuinely elevated mortality during exacerbations. Evidence-based management strategies for bronchitis slow this structural decline most effectively when initiated in the earlier stages of disease — waiting for symptoms to become disabling before seeking structured care consistently produces worse outcomes. Patients who incorporate low-impact cardiovascular conditioning, such as regular use of a stair stepper for cardiopulmonary fitness, often maintain better functional lung capacity alongside medical management.
From a purely financial standpoint, delayed treatment converts a low-cost outpatient visit into a high-stakes hospital admission. The cost differential between early and late intervention is not marginal — it spans orders of magnitude sufficient to create lasting financial hardship, entirely independent of the health consequences.
| Disease Stage | Typical Intervention | Estimated Cost (USD) | Average Recovery Time |
|---|---|---|---|
| Acute bronchitis — early, outpatient | Physician visit, symptomatic management | $150 – $350 | 10–21 days |
| Acute bronchitis with secondary infection | Physician visit, antibiotics, chest imaging | $400 – $900 | 3–5 weeks |
| Bronchitis progressing to pneumonia | ER evaluation, possible hospitalization | $3,000 – $15,000 | 4–8 weeks |
| Chronic bronchitis acute exacerbation (COPD) | Hospital admission, bronchodilators, oxygen therapy | $8,000 – $35,000+ | Ongoing management |
These figures represent the direct financial argument for early medical attention, completely separate from the clinical argument. High-deductible insurance plans leave many patients absorbing thousands in out-of-pocket costs for what was a preventable escalation — a predictable consequence of the systemic tendency to rationalize respiratory symptoms as temporary inconveniences rather than warning signals.
For patients managing chronic respiratory conditions or recovering from acute bronchitis at home, consistent blood oxygen monitoring represents one of the highest-value preventive investments available. Readings consistently below 95 percent saturation warrant physician consultation; readings below 90 percent require emergency evaluation without delay. Chronic cough also imposes significant mechanical stress on the thoracic and lumbar spine, and patients experiencing lower back pain alongside respiratory symptoms should communicate both to their physician, since prolonged severe coughing strains the paraspinal musculature in ways that complicate overall recovery and rehabilitation.
Medical misinformation about bronchitis is pervasive, and several persistent myths directly contribute to the dangerous treatment delays that convert manageable illness into medical crisis. These misconceptions are not harmless — they have measurable downstream consequences for patient outcomes.
This belief holds partial accuracy for healthy adults under 65 with acute viral bronchitis, but it becomes dangerous when applied universally. Patients over 65, those with asthma, and those with diminished lung reserve cannot rely on the same self-resolution timeline as a healthy young adult. Beyond the acute phase, many patients who stop coughing retain subclinical airway inflammation that quietly progresses to structural remodeling over subsequent months. The disappearance of symptoms does not equal the resolution of underlying disease — a distinction that clinicians encounter repeatedly in patients presenting with advanced chronic bronchitis who dismissed each prior acute episode as self-limiting and temporary.
Because bronchitis produces thick, discolored mucus and systemic malaise, patients frequently assume bacterial infection and expect antibiotic prescriptions. Clinically, viral agents — primarily rhinovirus, influenza, and coronavirus strains — account for the vast majority of acute bronchitis cases, and antibiotics offer zero benefit against viral pathogens. Appropriate management focuses on bronchodilators when airflow obstruction is present, structured rest, adequate hydration to support mucociliary clearance, and follow-up evaluation to detect any secondary bacterial infection early. Prescribing antibiotics indiscriminately accelerates resistance without addressing the underlying pathogen, a pattern that public health authorities have documented extensively as a contributor to treatment-resistant respiratory infections.
The gap between a routine bronchitis diagnosis and a fatal outcome is almost always bridged by identifiable, preventable errors in self-management. These are not rare or exotic mistakes — they are the same patterns clinicians encounter repeatedly across patient populations and demographic groups.
The most dangerous error is treating escalating breathlessness as an expected feature of the illness rather than a clinical alarm signal. Patients who rationalize increasing dyspnea as "just how bronchitis feels" frequently delay emergency contact until oxygen saturation has dropped to levels requiring intensive intervention. The clinical standard is straightforward: any bronchitis symptom that worsens after the first seven days demands medical re-evaluation without exception. Disrupted sleep from respiratory symptoms also compounds immune suppression significantly — quality rest is a physiological requirement during respiratory illness, not a secondary comfort preference, as research on managing sleep in chronic inflammatory conditions consistently demonstrates.
Over-the-counter cough suppressants, used incorrectly during productive-cough phases, impair mucociliary clearance and trap infectious material in the airways — creating an environment where bacterial colonization accelerates. Similarly, patients using leftover antibiotics from previous prescriptions introduce both dosing inaccuracies and resistance-selection pressure without the benefit of appropriate diagnostic confirmation. Bronchitis management that deviates from physician-directed care — particularly in patients with existing cardiovascular or pulmonary disease — carries measurably higher complication rates across the published clinical literature.

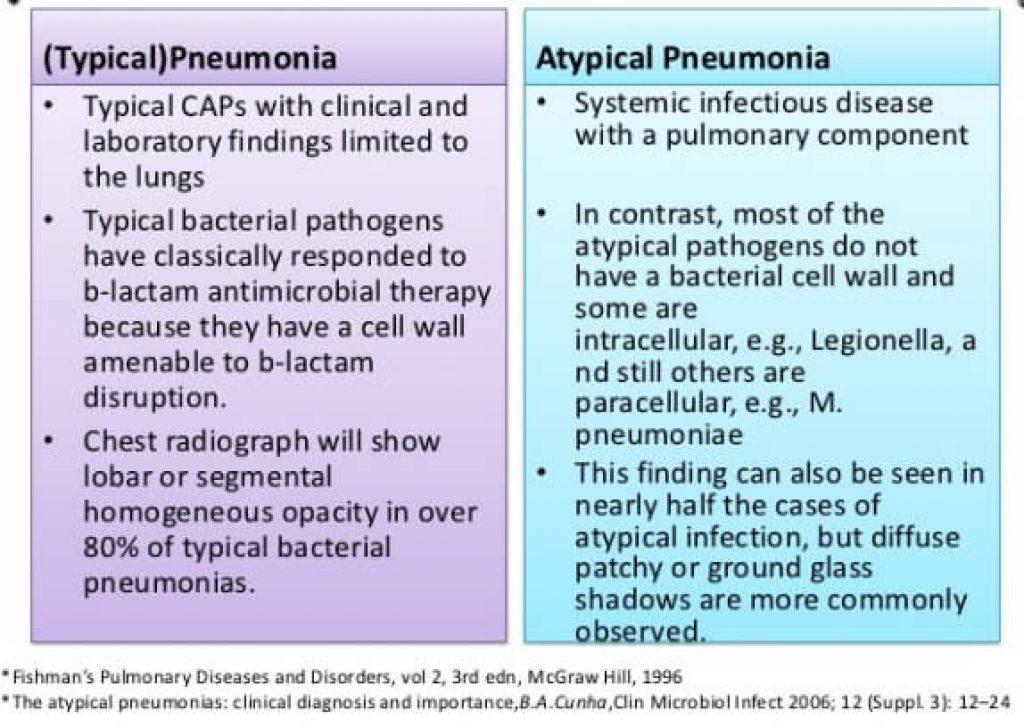
The distinction between bronchitis and pneumonia is one of the most consequential differentiations in respiratory medicine, and confusion between the two has contributed directly to fatal delays in appropriate care. The two conditions share overlapping symptoms — cough, fever, chest discomfort — but differ fundamentally in anatomical site, diagnostic criteria, and mortality profile.
Bronchitis affects the bronchial tubes themselves; pneumonia involves the alveolar air sacs where gas exchange actually occurs. This anatomical distinction matters because infected alveoli physically reduce functional lung tissue and create the conditions for hypoxemia — dangerously low blood oxygen — that uncomplicated bronchitis rarely produces in otherwise healthy lungs. Chest X-ray remains the definitive differentiating tool, revealing consolidation or infiltrates in pneumonia cases that are absent in pure bronchitis. According to the Centers for Disease Control and Prevention, pneumonia accounts for over one million hospitalizations annually in the United States, a significant proportion of which originate from inadequately managed bronchitis that crossed into alveolar infection.
The transition occurs when bacterial colonization of inflamed airways spreads distally into the alveoli. This progression is most common in patients who suppress productive coughing prematurely with suppressants, fail to maintain hydration adequate for mucociliary clearance, or have immune responses that cannot contain the initial bacterial load. Fever spiking above 103°F (39.4°C), marked increase in breathlessness, and sharp pleuritic chest pain are the hallmark clinical signals of this transition. Patients who recognize these indicators and present for evaluation within 24 hours of onset consistently demonstrate better outcomes than those who delay for a follow-up appointment scheduled days later.
Death from bronchitis in healthy adults under 65 is uncommon but not impossible. The primary fatal risk comes from downstream complications — bacterial pneumonia, respiratory failure, or sepsis — rather than from uncomplicated acute bronchitis itself. Maintaining adequate hydration, monitoring symptom trajectory, and seeking medical evaluation at the first sign of deterioration effectively eliminates this risk in patients with no significant underlying health conditions.
Symptoms that persist beyond three weeks, worsen after the first seven days, or include high fever, blood-streaked sputum, or significant breathlessness require medical evaluation regardless of how much time has elapsed. High-risk patients — those over 65, active smokers, or individuals with pre-existing lung disease — should seek evaluation within the first week rather than relying on a standard self-resolution window that applies to healthier populations.
Bacterial pneumonia is the most common life-threatening complication of untreated bronchitis, particularly in elderly and immunocompromised patients. The inflamed bronchial environment provides an optimal substrate for bacterial colonization that can extend distally into the alveoli, causing consolidation, progressive hypoxemia, and in severe cases, septicemia requiring intensive care-level intervention. Early detection through monitoring and prompt medical response is the most effective prevention strategy.
Advanced chronic bronchitis as a component of COPD is associated with reduced life expectancy, particularly when forced expiratory volume falls below 50 percent of predicted values. The degree of reduction depends on smoking cessation status, frequency of acute exacerbations, adherence to pulmonary rehabilitation, and management of comorbid cardiovascular conditions. Patients who cease smoking and engage with structured management programs demonstrate markedly better survival curves than those who continue smoking or forgo structured care.
Repeated insufficiently treated episodes of acute bronchitis can contribute to progressive airway remodeling and mucociliary dysfunction over time. Chronic bronchitis, by definition, involves structural changes to the airway walls — glandular hypertrophy and goblet cell hyperplasia — that are not reversible once established. This irreversibility is the primary clinical argument for aggressive early management of every acute episode, rather than the passive monitoring approach that patients often default to when symptoms appear mild in isolation.





About Mehmet Kesimer, PhD
Mehmet Kesimer is an associate professor of pathology and laboratory medicine at the University of North Carolina at Chapel Hill, based at the Marsico Lung Institute. His research specializes in mucin biology and airway defense mechanisms, with a particular focus on how dysfunction in these systems contributes to chronic lung diseases including COPD, cystic fibrosis, and asthma. He collaborates closely with Dr. Richard C. Boucher and has published foundational research establishing mucin concentration as a diagnostic marker for chronic bronchitis and COPD progression.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below