
Around 5 percent of acute bronchitis cases progress to pneumonia — and that number climbs sharply for adults over 65, smokers, and anyone with a compromised immune system. If your cough has stretched past ten days and symptoms seem to be intensifying rather than fading, you could already be facing bronchitis turning into pneumonia. The two conditions look deceptively similar on the surface, but they require completely different treatment approaches. Start with our bronchitis resource hub for a full overview, then read on — catching this transition early can make a significant difference in your recovery.
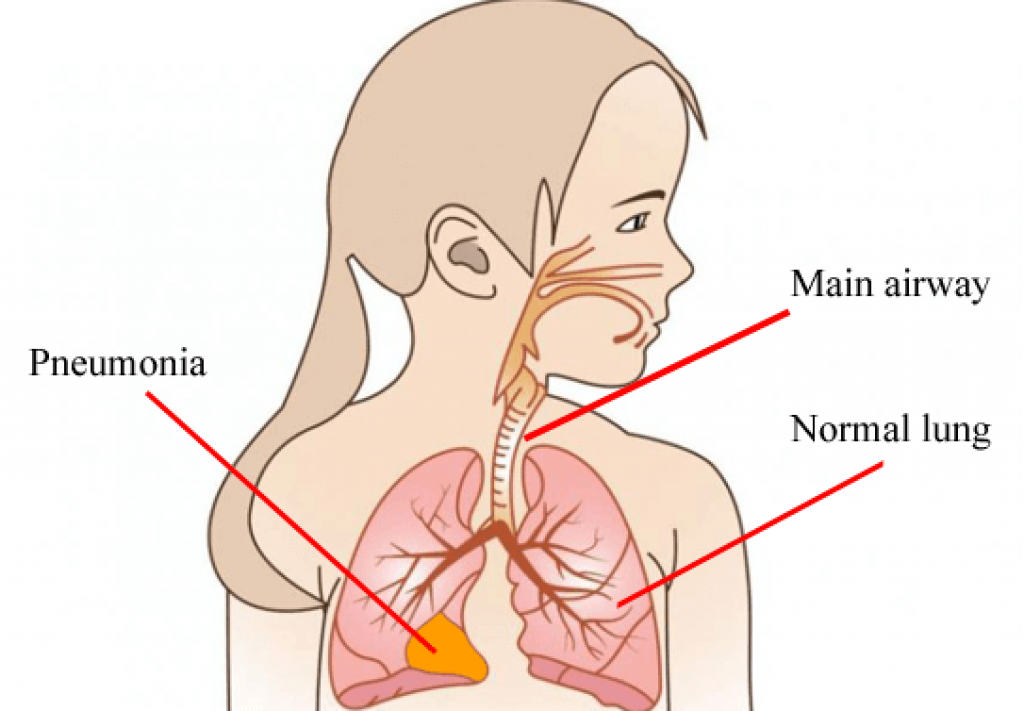
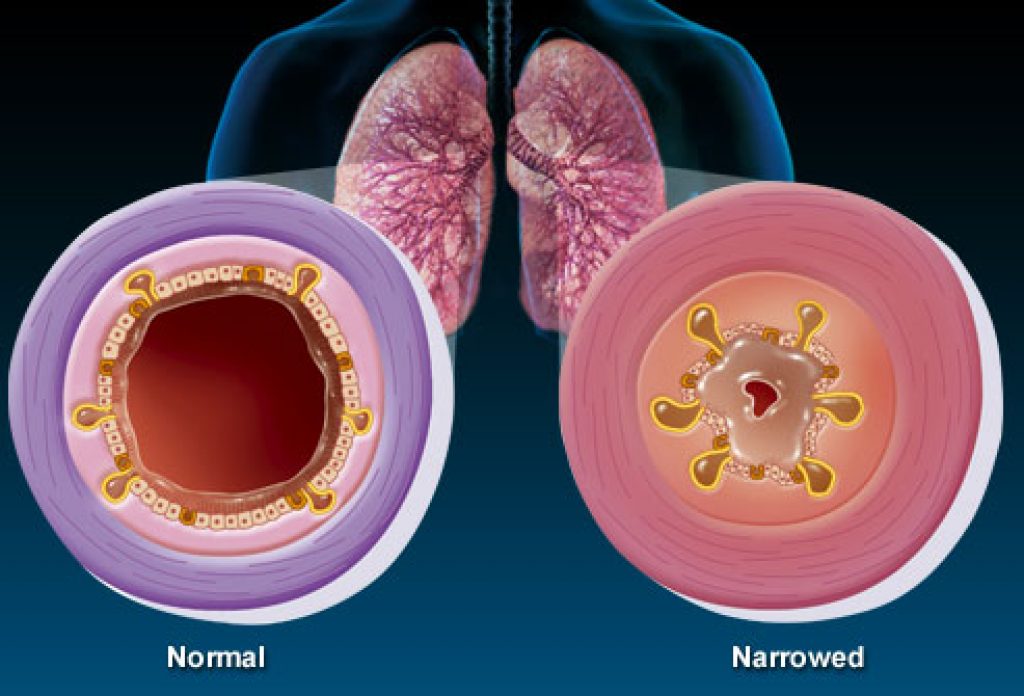
Bronchitis inflames the bronchial tubes — the airways that carry air into your lungs. Your immune system typically clears the viral infection within ten to fourteen days. The catch is that those irritated, swollen airways create the perfect environment for a secondary bacterial infection to take hold. That's the moment bronchitis can cross the line into pneumonia, which infects the air sacs deep in your lungs and begins filling them with fluid or pus.
Pneumonia doesn't just feel worse — it behaves differently. Breathing becomes painful. Oxygen exchange drops. For vulnerable people, it can spiral into a life-threatening situation within days. Understanding where bronchitis ends and pneumonia begins means you can catch that transition early, get the right treatment, and avoid a much harder road to recovery.
Contents
Most cases of acute bronchitis are self-limiting. Your body fights the virus, inflammation settles down, and within two weeks you're back to normal. But there's a critical window where waiting becomes a mistake. Knowing how to read your own symptoms tells you whether you should stay home and rest — or get to a doctor before something more serious takes hold.
These signs typically point to uncomplicated bronchitis that your immune system can handle on its own:
If your symptoms match this pattern, standard bronchitis care applies: rest, plenty of fluids, over-the-counter cough suppressants, and steam inhalation for relief. You almost certainly don't need antibiotics at this stage — and taking them when you don't need them is actually counterproductive. If you're wondering about the more serious end of the spectrum, our article on whether bronchitis can become life-threatening without treatment covers what untreated cases can look like.
These symptoms call for immediate medical attention. Don't try to wait them out at home:
If your fever breaks and then comes back stronger after a day or two, that pattern is a classic warning sign of a secondary bacterial infection establishing itself in your lungs — the exact transition you want to catch early.
Pneumonia can deteriorate surprisingly fast, particularly in older adults and those with underlying conditions. When you see these warning signs, you're no longer in "wait and see" territory.
The symptoms of bronchitis and pneumonia overlap in ways that make them genuinely difficult to distinguish at home. You can feel seriously ill either way — but what's happening inside your respiratory system is quite different, and that difference determines everything about how you should be treated.
Here's how the two conditions compare against each other and against influenza, which often triggers both:
| Flu/ Influenza | Bronchitis | Pneumonia | |
| Cause | Caused by Influenza A or B virus. | Caused by virus from the developed stage of common cold. | Caused by both virus and later by bacteria. |
| Affects | Affects respiratory system. | Inflames air sacs of lungs. | Infects air sacs of lungs. |
| Symptoms | Symptoms are high fever, muscle ache, persistent cough, nasal congestion, sore throat, etc. | Hard time breathing, coughing with wheezing sound, muscle ache, etc. | Chest pain, confused mental awareness, cough with phlegm, fatigue, chills, etc. |
| Duration | May last from 1 to 3 weeks. | May last for 10-14 days or more than 3 weeks. | May last for 3 weeks or carry on for a lifetime. |
| Treatment | Enough bed rest and fluid in normal cases but prescribed antiviral medicines in complicated conditions. | Enough rest and fluid, cough suppressant medicines, pain reliever medicines, etc. Antibiotics for bacterial bronchitis. | Enough bed rest, healthy lifestyle, nutritious diet, vaccinations, prescribed medicines, etc. |
| Severity | It may go away on its own but can be life-threatening for victims with weak immune system. | Acute bronchitis is curable within 3 weeks at best but chronic bronchitis may last for a lifetime. | A worldwide phenomenon disease that affect about a million people in the US only. |
And here's how bronchitis differs from the common cold that often precedes it:
| Bronchitis | Cold | |
| Cause | Caused by viral or bacterial infection in the lungs. | Caused by viral attack in the respiratory system. |
| Affect | Inflames air sacs of lungs. | Affects nasal line, throat, and chest. |
| Treatment | May go away on its own if it's viral but may need antibiotics if it's a bacterial bronchitis. | Since, caused by virus, antibiotics are not applicable. OTC medicines may be helpful in comforting irritations and achiness. |
| Duration | Not life compromising but may be lifelong suffering. | Infectious from one to another and go away on its own within one week or two. |
At home, you can't reliably distinguish early pneumonia from bronchitis based on how you feel alone. When you visit a doctor with a suspected respiratory infection, here's what to expect:
Most bronchitis does not require antibiotics. Since the vast majority of cases are viral in origin, antibiotics have no effect on the pathogen causing the infection. Pneumonia, by contrast, typically needs a targeted antibiotic course — and sometimes hospitalization, depending on severity. The following table lays out the practical differences clearly:
| SL No | Bronchitis | Pneumonia |
| 1 | Bronchitis is a viral infection that often accompanies the common cold. | Pneumonia is a bacterial infection that causes fluid to escape into the lungs. |
| 2 | Typically bronchitis can resolve on its own within a week or two. | Patients with pneumonia will likely need an antibiotic. |
| 3 | Usually with bronchitis you do not need antibiotics as it's a viral illness and it will resolve on its own and actually giving antibiotics can be a bad thing you're exposing different bugs to the antibiotics and that's how you get resistances. | If pneumonia is left untreated it can become very severe even life-threatening for children and the elderly. |
| 4 | A lot of people will get pneumonia with bronchitis especially if their immune system for whatever reason is already kind of compromised. | If a patient has pneumonia symptoms it's important they visit their doctor to be diagnosed patients with asthma or COPD may need more aggressive treatment to prevent the diagnosis from getting worse. |
Treating yourself for bronchitis when you actually have pneumonia isn't just ineffective — it's dangerous. The bacterial infection continues progressing while you rest at home and assume it will pass on its own.
Not everyone with bronchitis faces the same level of risk. Some people clear the infection without incident. Others — because of age, lifestyle, or underlying conditions — are far more vulnerable to that dangerous shift into pneumonia.
These are the people who need to monitor symptoms most carefully when bronchitis strikes:
People managing chronic fatigue conditions — including fibromyalgia — may also be more susceptible. When your immune system is already working under strain, respiratory infections can hit harder and last longer. Some evidence supports that targeted nutritional support can help maintain immune resilience; you can explore that angle in our guide on fibromyalgia supplements that may help boost energy and immune function.
Understanding real-world patterns helps you recognize when you — or someone close to you — might be heading toward pneumonia rather than recovering from bronchitis.
Case 1 — The elderly patient who waited too long: A 70-year-old woman develops what looks like a typical winter cold. After a week, her cough deepens and she develops a low-grade fever. Her family assumes she's still fighting the virus. By day ten, she's breathing shallowly and seems confused — signs of walking pneumonia that had been progressing undetected. A chest X-ray confirms bilateral pneumonia requiring hospitalization.
Case 2 — The longtime smoker in his 40s: A 44-year-old smoker gets bronchitis most winters. This year starts the same way. But by day eight, his mucus turns greenish-yellow and chest tightness develops. Because his airways are already damaged by years of smoking, the bacterial load overwhelms his defenses faster than it would in a healthy adult. He needs IV antibiotics and several days of inpatient care.
Case 3 — The person who returned to work too early: A 35-year-old feels noticeably better after five days of bronchitis and heads back to a demanding job. Within 48 hours the fever returns — higher than before — and chest pain develops. Physical and emotional stress during an active infection is a well-documented factor in immune suppression and secondary infection risk.
These cases aren't outliers. According to the CDC, pneumonia accounts for over 1.5 million emergency room visits in the United States annually — many of them preventable with earlier intervention.
There's a surprising amount of misinformation circulating about respiratory infections. These myths lead people to make poor decisions about when to seek care — and sometimes those decisions carry real consequences.
This one generates unnecessary panic. The reality is that most acute bronchitis cases — particularly in otherwise healthy adults — resolve completely without ever progressing to pneumonia. The overall risk figure is around 5 percent across the full population; for a healthy young adult with no underlying conditions, the odds are considerably lower. Bronchitis turning into pneumonia is a risk to manage, not a foregone conclusion.
The key is knowing your personal risk profile and actively watching for the specific warning signs rather than assuming every respiratory infection will spiral. Two more myths worth addressing quickly:
This may be the most consequential myth on the list. Many people request antibiotics at the first sign of bronchitis, believing they'll prevent progression to something worse. But since most bronchitis is viral, antibiotics have no effect on the pathogen causing it. Worse, unnecessary antibiotic use:
Antibiotics are appropriate and necessary when bacterial pneumonia has been confirmed. Using them preemptively against viral bronchitis doesn't accelerate recovery — it creates new problems.
Even people who know the warning signs sometimes make decisions that give the infection room to progress. These are the most consistent missteps seen in bronchitis-to-pneumonia cases — and how to avoid them.
Feeling better for a single day doesn't mean you're recovered. This is one of the most common patterns in cases where bronchitis progresses to pneumonia. When you get a brief lift in symptoms, your immune system is still actively fighting the infection. Returning to work, resuming intense exercise, or cutting rest short diverts energy away from healing and leaves the door open for bacterial superinfection.
This is also worth noting for anyone managing concurrent musculoskeletal issues — prolonged, forceful coughing puts real strain on the chest, ribcage, and back. If you're dealing with that kind of secondary discomfort, our guide on lower back pain causes and treatment covers approaches that can help while you recover. Give yourself genuine rest, not just reduced activity.
A cough that persists beyond three weeks is no longer "just bronchitis." Many people avoid the doctor because they assume they're still clearing the original viral infection — or they don't want to be told to wait it out. But by week three, a secondary bacterial infection may already be active and established.
A basic pulse oximeter — available at most pharmacies — can provide useful information at home. If your blood oxygen saturation drops below 95 percent, that's a cue to get evaluated regardless of how you otherwise feel.
Whether this is your first respiratory infection or your fifth, the experience of bronchitis — and the risks that come with it — shifts considerably depending on your history. What applies to a healthy first-timer is different from what someone with recurring bronchitis needs to understand.
If you've never had bronchitis before, you don't have a reference point for how it should feel or how it typically progresses. That actually works in your favor in some ways — you're less likely to dismiss warning signs because "this is just how it always feels for me."
For a first episode, keep these expectations in mind:
What isn't normal: symptoms that reverse course after appearing to improve. If you feel clearly better on day six and noticeably worse on day eight, that reversal is the specific pattern that warrants a call to your doctor. Don't rationalize it as "just a setback."
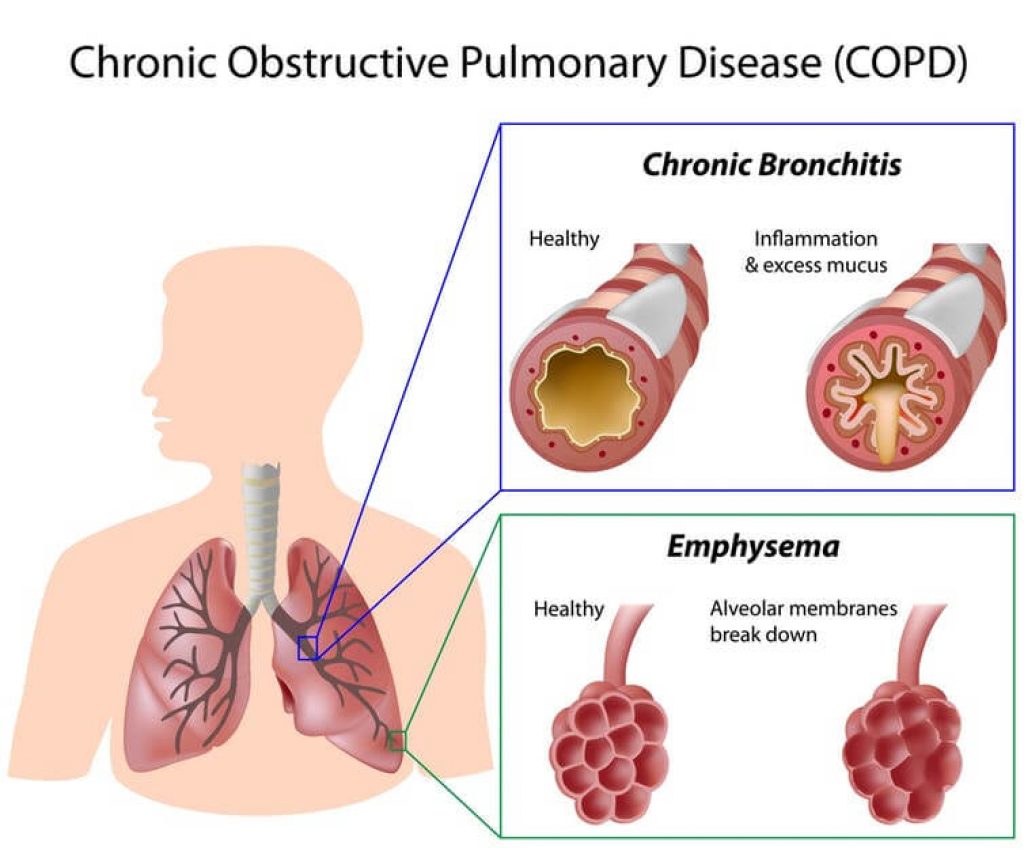
Recurrent bronchitis — more than two or three episodes per year — is a red flag in itself. It may indicate chronic bronchitis, which is classified as a form of COPD (Chronic Obstructive Pulmonary Disease). People with chronic bronchitis have persistently inflamed airways that make them significantly more susceptible to pneumonia during any acute flare, and their symptoms at baseline can mask the early signs of a more serious infection.
If you experience bronchitis repeatedly, these steps apply directly to you:
Experienced patients often normalize symptoms that genuinely need attention. More history with bronchitis should make you more alert to changes, not more comfortable dismissing them.
Yes, in some cases it can — particularly for high-risk individuals. While the transition typically develops over a week or more, people with weakened immune systems, COPD, or significant underlying conditions can experience rapid progression within 48 to 72 hours. That's why daily symptom monitoring during any active bronchitis episode is worth the effort, especially if you fall into a high-risk category.
Pneumonia tends to feel far more systemic than bronchitis. With bronchitis, the cough is usually the dominant complaint. With pneumonia, you're typically dealing with chest pain that sharpens when you breathe deeply, a high fever, shortness of breath even at rest, and a level of fatigue that feels genuinely crushing rather than just tiring. Mental confusion or unusual disorientation — especially in older adults — is a pneumonia-specific symptom that rarely appears with uncomplicated bronchitis.
For most adults who can still breathe adequately and are not in acute distress, urgent care is appropriate — it can handle a chest X-ray, blood work, and an antibiotic prescription. Go directly to the emergency room if you experience severe shortness of breath at rest, blood oxygen below 90 percent, significant confusion or altered mental state, lips or fingernails turning blue, or chest pain that has a cardiac quality to it.
No — the pneumococcal vaccine targets pneumonia caused by Streptococcus pneumoniae specifically, which is the most common bacterial cause. It does not protect against viral pneumonia or pneumonia caused by other bacterial strains. That said, it significantly reduces your risk of the most serious and most common form of bacterial pneumonia, and it is strongly recommended for adults over 65, smokers, and anyone with chronic lung, heart, or immune conditions.
Bronchitis turning into pneumonia is a real risk — but it's one you can manage with the right information and timely action. Track your symptoms day by day, take your temperature once daily, and don't rationalize warning signs because you expect to feel better soon. If your fever returns after breaking, your breathing becomes labored, or chest pain develops, contact your doctor that same day — don't wait for the situation to become obvious. Your lungs are worth the call.





About Mehmet Kesimer, PhD
Mehmet Kesimer is an associate professor of pathology and laboratory medicine at the University of North Carolina at Chapel Hill, based at the Marsico Lung Institute. His research specializes in mucin biology and airway defense mechanisms, with a particular focus on how dysfunction in these systems contributes to chronic lung diseases including COPD, cystic fibrosis, and asthma. He collaborates closely with Dr. Richard C. Boucher and has published foundational research establishing mucin concentration as a diagnostic marker for chronic bronchitis and COPD progression.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below