
What would happen if a small blister on your foot went unnoticed for weeks? For people living with diabetes, that scenario can escalate into a serious infection — or worse. Diabetes foot checks prevention is not a routine afterthought; it is one of the most consequential habits you can build for your long-term health. This guide breaks down exactly why these checks matter, what a thorough examination involves, and how to protect yourself from the complications that claim thousands of limbs each year. If you manage diabetes, this belongs in your foot care routine without exception.
Diabetes affects both the circulatory and nervous systems in ways that make foot problems uniquely dangerous. Peripheral neuropathy — nerve damage caused by chronically elevated blood glucose — dulls sensation in the feet. Cuts, blisters, and pressure sores that would ordinarily trigger immediate pain can go undetected for days. Poor circulation then slows healing, creating an environment where minor wounds become infected wounds, and infected wounds become surgical emergencies. According to the Centers for Disease Control and Prevention, diabetes is the leading cause of non-traumatic lower-limb amputations in the United States.
The encouraging reality is that the vast majority of diabetic foot amputations are preventable. Consistent self-examination, combined with regular professional assessments, catches problems while they are still manageable. The sections that follow walk you through every dimension of diabetic foot monitoring — from daily maintenance routines to advanced vascular screening. For a broader foundation, the guide on basic foot care tips for year-round exposure provides essential context that complements the diabetes-specific strategies presented here.
Contents
Diabetes does not damage the feet overnight. The damage accumulates silently across months and years of elevated blood glucose affecting nerve fibers and blood vessels. Understanding this progression is the first step toward interrupting it before irreversible harm occurs.
Peripheral neuropathy affects approximately 50% of people with diabetes and presents in three forms: sensory, motor, and autonomic. Sensory neuropathy removes your ability to accurately feel pain, heat, or pressure. Motor neuropathy alters gait mechanics, increasing abnormal loading on specific areas of the sole. Autonomic neuropathy reduces sweat production, leaving skin dry, brittle, and prone to fissure formation.
Moisturizing consistently addresses one of those vulnerabilities directly. A foot cream formulated for nerve damage and pain restores skin integrity and reduces the risk of surface-level wounds becoming entry points for infection.
Peripheral arterial disease (PAD) co-occurs with diabetes at a significantly higher rate than in the general population. Reduced arterial blood flow means oxygen and immune cells reach wound sites more slowly. A cut that heals in days for a non-diabetic person may remain open for weeks in someone with both neuropathy and compromised circulation. This combination — impaired sensation alongside impaired healing — is precisely what makes diabetic foot wounds disproportionately dangerous.
A daily foot inspection is the single most impactful action you can take for diabetes foot checks prevention. The process requires less than five minutes and no specialized equipment beyond what you already have.
If limited mobility prevents you from seeing the soles and heel areas, a long-handled mirror resolves the problem immediately. For those with significant flexibility limitations, consider reviewing the guidance on why seniors need regular podiatrist check-ups — professional examinations fill the gaps that self-checks cannot.
Document your findings consistently. A simple weekly photograph creates a visual baseline that reveals gradual changes that would otherwise go unnoticed between clinic visits.
Even well-intentioned patients make mistakes that accelerate foot complications. Recognizing these errors is as important as following correct protocols.
Ill-fitting footwear accounts for a substantial proportion of diabetic foot ulcers. Shoes that are too tight create sustained pressure on the metatarsal heads and lateral borders. Shoes that are too loose allow shearing forces that abrade the skin with every step. Sandals and open-toed shoes expose the foot to blunt trauma while providing no protective benefit.
Tip: Always shop for footwear in the afternoon when feet are at their largest, and have both feet measured professionally — foot dimensions frequently change with age and neuropathy-related muscle atrophy.
Soaking your feet in hot water is among the most common and damaging habits in diabetic patients. Neuropathy impairs your ability to gauge water temperature accurately; scalding injury can occur before you register any discomfort. Always test water temperature with your elbow before immersion.
Cracked heels are not merely cosmetic. Deep heel fissures serve as portals for bacterial entry and must be treated proactively. A detailed review of heel rescue foot creams and their effectiveness on fissures can guide your product selection. Cutting toenails too short — or at angles rather than straight across — creates ingrown nails that pierce adjacent skin, a significant ulcer risk in neuropathic feet.
| Complication | Early Warning Signs | Required Action |
|---|---|---|
| Peripheral Neuropathy | Tingling, numbness, burning sensation in feet | Neurological assessment; begin daily foot inspection |
| Diabetic Foot Ulcer | Open sore, redness, warmth, drainage | Immediate medical evaluation — do not delay |
| Peripheral Arterial Disease | Pale or bluish skin, cold feet, leg cramping | Vascular specialist referral |
| Charcot Foot | Sudden swelling, redness, warmth, structural deformity | Emergency podiatric care |
| Fungal Infection (Tinea Pedis) | Scaling, itching, macerated skin between toes | Topical antifungal; keep inter-digital spaces dry |
| Ingrown Toenail | Pain, redness, swelling at nail border | Podiatrist visit; do not attempt self-treatment |
Not every protective measure requires a clinic visit. Several high-impact habits take under ten minutes per day and meaningfully reduce your overall risk profile.
Anchoring these checks to an existing habit — immediately after brushing your teeth, for example — dramatically improves long-term adherence without requiring additional mental scheduling.
Poor circulation is addressable through targeted lifestyle interventions. Wearing compression socks designed for swollen feet supports venous return and reduces the edema that contributes to skin breakdown. Pairing this with daily low-impact movement maintains arterial blood flow throughout the lower extremities. The exercises for building strong and healthy feet covered in our dedicated guide are particularly suited to diabetic patients who need to maintain foot strength without high-impact loading risk.
Self-care and professional care are not alternatives — they are complementary layers of a single protective strategy. The following approaches represent evidence-based practices endorsed by podiatric and endocrinological professional organizations.
A comprehensive clinical foot examination includes several assessments that self-checks cannot replicate:
These tests should occur at least annually for all diabetic patients, and every three to six months for those with established neuropathy or a prior ulcer history.
Custom orthotic insoles redistribute plantar pressure away from high-risk zones — typically the first metatarsal head and the posterior heel. They are not interchangeable with over-the-counter insoles. A podiatrist uses pressure-mapping technology to identify your specific loading pattern before fabricating a device. For those who also manage arch-related discomfort, supportive hosiery is a meaningful adjunct to orthotic use. The comprehensive review of plantar fasciitis socks covers options that pair effectively with prescribed orthotic devices.
Clinical Note: Patients with a prior diabetic foot ulcer face a recurrence rate exceeding 40% within three years. A custom orthotic program combined with therapeutic footwear is the most effective evidence-based intervention for preventing that recurrence.
Both self-checks and professional exams serve distinct and irreplaceable purposes. Understanding where one ends and the other begins prevents both complacency and unnecessary alarm.
You observe your feet 365 days per year. No clinic appointment schedule can match that surveillance density. Daily self-examination detects:
The effectiveness of self-checks depends entirely on consistency and technique. Performed correctly every day, they form the most powerful first line of defense available to you.
Self-checks have clear and fixed limitations. You cannot perform monofilament testing on yourself. You cannot evaluate your ankle-brachial index. You cannot assess the structural integrity of a healing ulcer with the naked eye alone. Certain findings — open wounds, areas of blackening, localized warmth with no visible injury, sudden-onset swelling — require same-day or next-day professional evaluation, not a wait-and-see approach.

The intensity of your monitoring protocol should match your individual risk level. A newly diagnosed patient with well-controlled blood glucose has fundamentally different needs than someone with a decade of neuropathy and a prior ulcer history.
If you are new to structured foot monitoring, begin with these foundational actions:
High-risk patients — those with established neuropathy, PAD, prior ulceration, or structural foot deformities — require an escalated approach:
High-risk patients should also revisit their exercise strategy. Low-impact options that avoid excess plantar loading — swimming, seated cycling, or recumbent bike sessions — maintain cardiovascular health without aggravating foot stress. Whatever your risk level, a consistent commitment to diabetes foot checks prevention remains the cornerstone of avoiding the most severe outcomes.
You should inspect your feet visually every single day. Daily checks allow you to detect acute injuries, developing pressure sores, and early-stage infections between scheduled clinical appointments. Consistency is more important than the duration of each check — sixty seconds of attentive inspection daily outperforms an occasional thorough review.
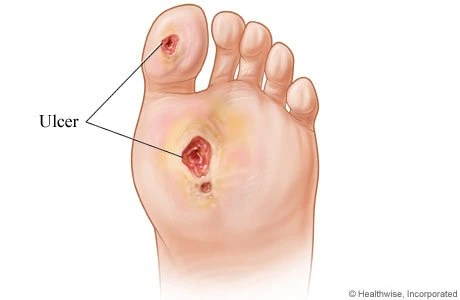
Early-stage diabetic foot ulcers typically present as shallow open sores with a red or pink wound bed, often surrounded by a ring of callused or thickened skin. The surrounding tissue may appear warmer than adjacent areas. Because neuropathy dulls pain sensation, you may notice the wound visually before you feel any discomfort — which is precisely why daily visual inspection is essential.
Mild neuropathy progression can be slowed or stabilized through rigorous blood glucose management, but established nerve damage does not fully reverse. Vascular complications similarly respond to lifestyle intervention and medical therapy but are not completely reversible. The most effective strategy is preventing initial damage through consistent diabetes foot checks prevention practices before complications develop.
No, but it is the most common contributing factor. Some patients develop foot ulcers primarily through ischemia — severely restricted arterial blood flow — without significant neuropathy. Others have both conditions simultaneously, which represents the highest-risk scenario. A clinical assessment that tests both sensation and vascular flow is necessary to determine which mechanism is dominant in your specific case.
Diabetic-specific therapeutic footwear features a deep, wide toe box, seamless interior lining, cushioned insole, and a rigid rocker-bottom sole to reduce forefoot loading. Your footwear should be professionally fitted, never purchased by online size alone. For those with significant neuropathy or prior ulcers, a podiatrist can prescribe custom-molded shoes that accommodate individual foot architecture precisely.
Chronically elevated glucose glycates proteins in nerve myelin sheaths, impairing nerve conduction velocity and eventually destroying nerve fibers. Simultaneously, elevated glucose damages the endothelial lining of small blood vessels, reducing their ability to dilate and deliver adequate oxygen to peripheral tissues. Both mechanisms proceed concurrently, which is why the feet — the furthest point from the heart — are disproportionately vulnerable.
Absolutely. The absence of pain is not a reliable indicator of foot health in someone with neuropathy — it may simply mean that the nerves capable of signaling pain have already been damaged. Annual professional foot exams detect monofilament sensation loss, early vascular compromise, and structural abnormalities long before they produce symptoms or visible wounds. Waiting for symptoms to appear is a strategy that leads to preventable complications.
Charcot neuroarthropathy — also called Charcot foot — is among the most destructive complications, involving progressive destruction of bone and joint architecture in a neuropathic foot. It frequently presents as sudden warmth, redness, and swelling without significant pain, and is commonly misdiagnosed as infection or sprain. Untreated Charcot foot leads to severe deformity and dramatically increases ulceration and amputation risk.





About Mehnaz
Mehnaz is the founder and editor of RipPain, a health resource site dedicated to helping readers navigate pain management, recovery, and medical device research. Her work on the site is driven by personal experience caring for seriously ill family members, which led her to study evidence-based guidance from physicians, pain specialists, and published medical research. She curates and summarizes expert medical insights to make credible health information accessible to everyday readers.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below