
Have you ever taken that first step out of bed in the morning and felt a sharp, stabbing pain shoot straight through your heel? If so, you already know how disabling this condition can be — and understanding plantar fasciitis boot how it works is one of the most effective moves you can make toward real recovery. The core mechanism is straightforward: a boot holds your foot at roughly a 90-degree angle while you rest, keeping the plantar fascia in a sustained stretch so that the micro-tears causing your pain can heal in a lengthened position rather than tightening back up overnight. That's the concept. But what separates people who recover in six weeks from those who stay stuck in pain for six months is knowing how to use the boot correctly — and what to do around it. For a full picture of the condition, start with our plantar fasciitis resource hub.
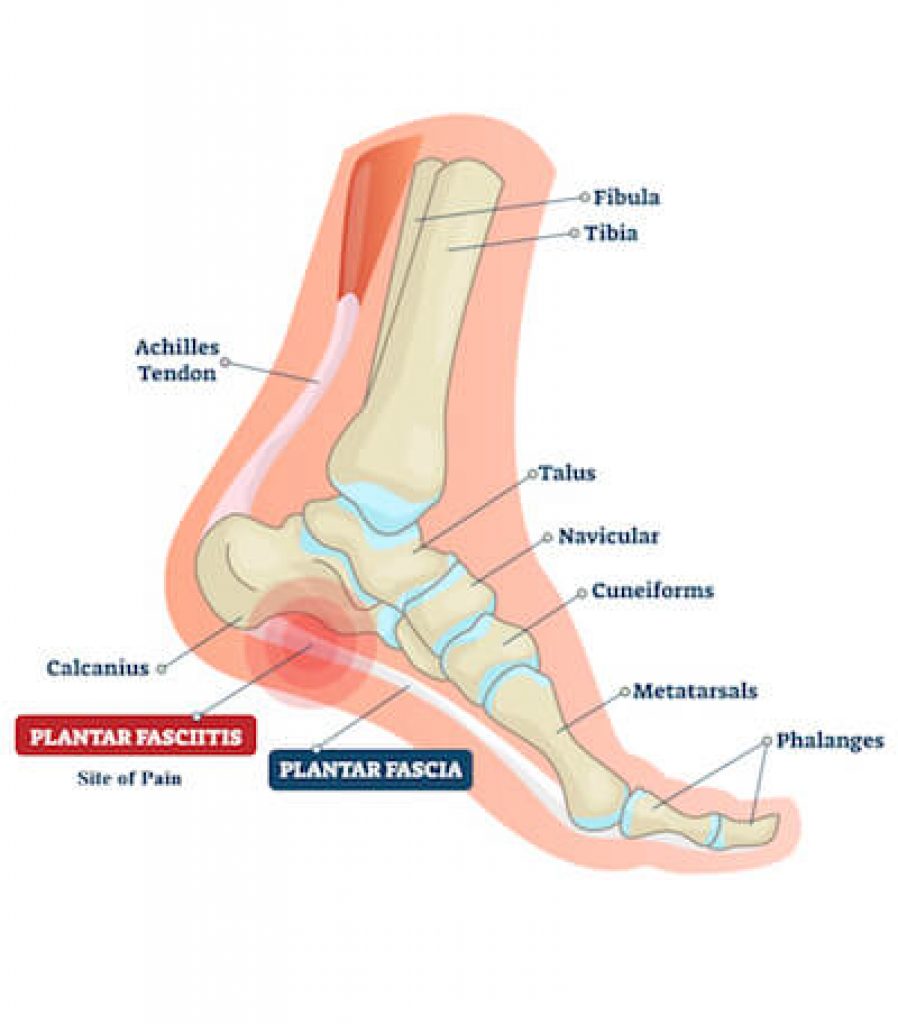
Plantar fasciitis develops when the thick band of connective tissue running from your heel bone to the base of your toes — the plantar fascia — is stressed and micro-torn faster than your body can repair it. Every time you rest, the fascia contracts and tightens. Every first step from bed yanks on that contracted tissue, causing the signature morning heel pain people describe as stepping on broken glass. Without targeted intervention, this cycle repeats indefinitely. You rest, the tissue tightens, you move, it tears again.
A plantar fasciitis boot breaks that cycle at its source. It isn't a standalone cure, and it won't do much if you strap it on and keep wearing unsupportive shoes all day. But combined with consistent stretching, proper footwear, and realistic expectations, it's one of the most evidence-backed conservative treatments available — recommended by podiatrists before cortisone injections, shockwave therapy, or surgery are ever considered. This guide covers the mechanics, the strategy, the common traps, the cost, and what to do when the boot alone isn't enough.
Contents
The pain you feel every morning has a specific mechanical cause. While you sleep, your foot naturally falls into a plantarflexed position — toes pointing downward, calf muscles shortened, plantar fascia fully contracted. When you bear weight on a cold, tightened fascia first thing in the morning, the already-damaged tissue gets re-injured before it ever had a chance to heal. This is why plantar fasciitis can persist for a year or more without treatment: rest doesn't mean recovery if the tissue is contracting every night.

Understanding plantar fasciitis boot how it works comes down to one principle: sustained dorsiflexion. The boot holds your ankle at approximately 90 degrees — or a few degrees past neutral — throughout the hours your foot isn't bearing weight. This keeps the plantar fascia and the calf muscles in a lengthened state, allowing healing to occur without the tissue snapping back to a shortened, contracted position by morning. Research reviewed by the National Institutes of Health found that patients using night splints consistently reported significant reductions in first-step morning pain compared to those relying on stretching exercises alone. The sustained stretch is the mechanism — and consistency over weeks, not days, is what produces results.
There are two distinct categories. Night splints are lightweight, designed exclusively for sleeping, and hold the ankle at or near 90 degrees without allowing weight-bearing. They come in two main forms: posterior splints, which cradle the back of the calf and heel, and dorsal splints, which sit on top of the foot and are generally more comfortable for sleep. CAM (controlled ankle motion) walking boots are a different tool — bulkier, designed for daytime use, and prescribed when the condition is severe enough that even normal walking is causing significant re-injury. For most people with mild-to-moderate plantar fasciitis, a night splint worn consistently for 4–8 weeks is the appropriate starting point. For a deeper breakdown of the condition itself and when each approach fits, our guide on Heel Pain and Plantar Fasciitis: Causes and Treatments provides useful diagnostic context.
Always perform 2–3 minutes of calf stretches and ankle pumps before putting your foot on the floor in the morning — skipping this step erases most of the progress your boot made while you slept.
The boot creates the right conditions for healing, but your habits around it determine how fast recovery actually happens. Most people put the boot on, tolerate it for a few nights, and assume they're done. Real results require a more deliberate approach.
Before you stand up each morning, flex your foot toward your shin 10–15 times, hold a towel-assisted stretch for 30 seconds, and follow up with a standing wall calf stretch. This warms the fascia after its night of sustained lengthening and prevents the "cold snap" re-injury that happens when you go straight from bed to walking. Evidence consistently shows that combining night splinting with targeted daily stretching cuts recovery time more effectively than either approach alone. Many patients also find that wearing compression socks during the day — particularly in the first few hours of activity — supports the arch and reduces inflammation between sessions. Our roundup of the Best Compression Socks for Plantar Fasciitis covers well-tested options that pair well with boot therapy.
A boot that's too tight restricts circulation and creates pressure points on your shin and heel. One that's too loose defeats the entire purpose — the ankle needs to be held firmly at 90 degrees, not allowed to drift into plantarflexion while you shift in bed. Straps should be snug but not cutting off sensation. Most people need 6–8 hours of nightly use to see meaningful improvement. If the boot is too uncomfortable to wear that long initially, start with 3–4 hours and build up over the first week. Your body needs time to adapt to the sustained stretch, and gradual compliance beats sporadic full-dose use.
This is where most people lose weeks — sometimes months — of potential recovery time. The boot is simple to use correctly, but the mistakes people make are equally simple and surprisingly common.
The most frequent problem is inconsistency. Wearing the boot two or three nights a week because it's uncomfortable produces almost no cumulative benefit. The tissue needs repeated, sustained lengthening over consecutive nights to shift the healing trajectory. Skipping nights resets much of your progress. On the opposite extreme, wearing a walking boot during all waking hours without medical guidance can cause muscle weakness and altered gait mechanics that create new problems. Use the right tool at the right time: night splint while sleeping, supportive shoes with orthotics while active.
Stopping the boot the moment your morning pain fades is the most common mistake patients make — that early relief is a sign the treatment is working, not that the fascia has fully repaired itself.
Your boot rehabilitates your foot during rest. What you wear while walking either reinforces or undoes that work. Flat shoes, flip-flops, and worn-out sneakers with no arch support subject the plantar fascia to the same mechanical stress that created the injury in the first place. If your job keeps you on your feet for long shifts, supportive footwear isn't optional — it's part of the treatment. Our guide to the Best Shoes for Nurses with Plantar Fasciitis was written for people in demanding, on-foot environments, but the principles apply to any occupation requiring extended standing. Even your off-duty footwear matters. During warmer months especially, reaching for unsupportive sandals can stall recovery significantly. The 15 Best Sandals for Plantar Fasciitis guide covers options with genuine arch support that don't compromise your daytime treatment.
One practical question almost everyone has before committing to boot therapy: is it worth the investment? The answer depends on what tier of boot fits your situation — and whether you qualify for insurance coverage.
| Boot Type | Price Range | Best For |
|---|---|---|
| Dorsal night splint (basic) | $20–$40 | Mild cases, first-time users, side sleepers |
| Posterior night splint | $30–$60 | Moderate cases, better ankle control |
| Adjustable night splint | $50–$90 | Customizable dorsiflexion angle, longer treatment |
| OTC CAM walking boot | $60–$130 | Acute flare-ups requiring daytime support |
| Prescription CAM walking boot | $150–$400+ | Severe or chronic cases, insurance-eligible |
The $30–$70 range covers the vast majority of patients with mild to moderate plantar fasciitis. Spending more buys adjustability and padding, not necessarily faster healing. A $45 boot you wear every single night outperforms a $200 boot worn sporadically. Comfort drives compliance, so if the posterior style keeps waking you up, switch to a dorsal splint — you're more likely to actually wear it.
If a podiatrist or orthopedist prescribes a boot, Medicare Part B and many private insurance plans cover it under durable medical equipment (DME) benefits — typically after a deductible and with a co-pay. Always request a written prescription before purchasing if you intend to file a claim. For over-the-counter boots, Health Savings Accounts and Flexible Spending Accounts recognize plantar fasciitis boots as qualified medical expenses, so you can use pre-tax dollars to purchase one. If cost is a factor, starting with a well-reviewed OTC night splint and escalating only if needed is a rational strategy.
Most patients see measurable improvement within 4–8 weeks of consistent boot use paired with stretching and supportive footwear. If you're past that window and your symptoms are unchanged — or worsening — something more is going on and the boot alone isn't going to resolve it.
Persistent pain after 8–10 weeks of dedicated conservative treatment is a clear indicator to see a podiatrist. Several conditions mimic plantar fasciitis closely enough to be misdiagnosed without imaging: tarsal tunnel syndrome, heel spurs, stress fractures, and nerve entrapment all produce heel and arch pain but require different interventions. If your pain has shifted from the heel toward the midfoot or ankle, or if you've developed knee or hip discomfort from compensating, you need a professional evaluation rather than more time in the boot. If a recent ankle injury preceded or coincided with your heel pain, treating the two separately often fails — an ankle sprain can alter gait mechanics in ways that directly worsen plantar fascia stress, and both need to be addressed together.
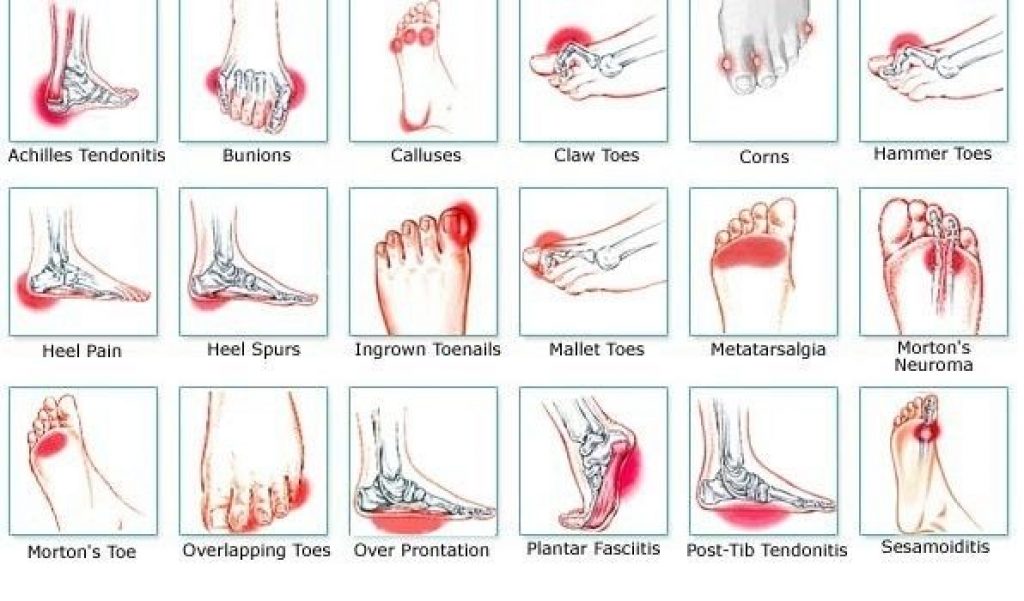
A boot is the conservative first line — not the ceiling of what's available. Physical therapy with eccentric heel-drop strengthening protocols, custom orthotics, extracorporeal shockwave therapy (ESWT), and corticosteroid injections are all validated options that can be layered in when boot therapy alone isn't sufficient. Your podiatrist will guide the sequencing based on how your tissue is responding. What matters is that you approach this systematically rather than cycling through random treatments without assessing what's working. The heel pain diagnosis chart above illustrates how different symptom patterns point toward different diagnoses — use it as a reference when talking with your provider about why recovery has stalled.
The boot only works as well as your commitment to wearing it — healing happens during the hours you keep it on, not the hours you decide it's too uncomfortable.





About Mehnaz
Mehnaz is the founder and editor of RipPain, a health resource site dedicated to helping readers navigate pain management, recovery, and medical device research. Her work on the site is driven by personal experience caring for seriously ill family members, which led her to study evidence-based guidance from physicians, pain specialists, and published medical research. She curates and summarizes expert medical insights to make credible health information accessible to everyday readers.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below