
Are you wondering why some women conceive with ease while others try for months without any luck? The truth is, the best fertility supplements for women can genuinely shift the odds in your favor — but only if you know which ones have real science behind them and how to use them correctly. This guide covers what to take, when to take it, what to avoid, and how to evaluate products worth your money. You'll also find a side-by-side comparison table and a breakdown of common myths that may be steering you in the wrong direction. For a broader look at evidence-based supplementation, visit our supplements section.
Fertility is shaped by a complex interplay of hormones, nutrition, stress levels, age, and genetics. No supplement changes all of that. But the right ones can correct deficiencies that directly affect egg quality, hormonal balance, ovulation regularity, and the uterine environment. The challenge is that the supplement market is flooded with products that mix a few well-researched ingredients with a lot of marketing hype. Knowing what actually belongs on your list — and what's mostly filler — is where this guide starts.
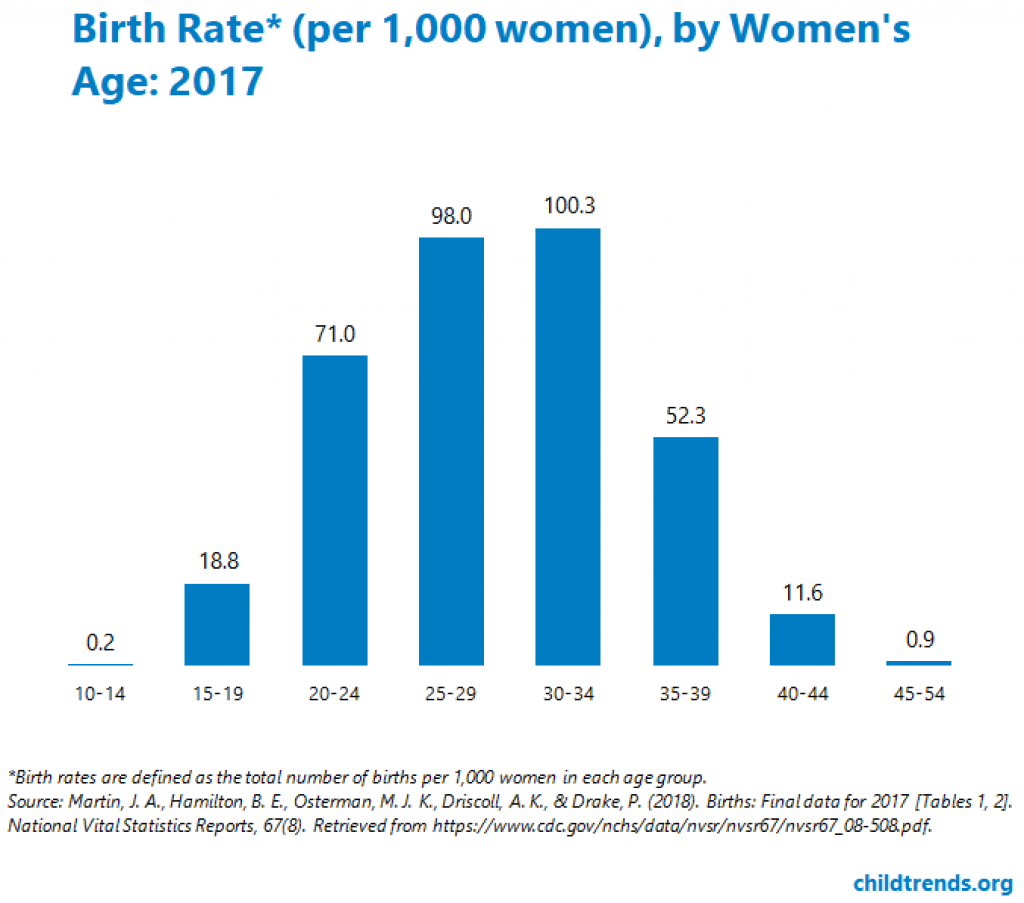
Fertility rates have been declining in many developed countries for demographic and lifestyle reasons. While supplementation isn't the answer to a population-wide trend, it can address individual nutritional gaps that make a real difference for women who are actively trying to conceive.
Contents
Not every supplement on a fertility shelf deserves to be there. A few, however, have enough research behind them that most reproductive specialists would agree they belong in the conversation. These are the ones worth understanding in depth before you spend money on anything else.

Folic acid is the synthetic form; folate is the naturally occurring version found in food. Both are forms of vitamin B9, and both matter for fertility. The CDC recommends that women of reproductive age take 400 micrograms of folic acid daily, beginning at least one month before trying to conceive. The reason this timing matters: neural tube development happens in the first few weeks after conception — often before a woman even knows she's pregnant. Women who carry the MTHFR gene variant may absorb methylfolate (the active form) more efficiently than standard folic acid. Ask your doctor whether genetic testing for this variant makes sense for you before committing to one form over the other.

CoQ10 is an antioxidant your body produces naturally, but levels decline with age — particularly after 30. Its role in mitochondrial energy production makes it directly relevant to egg quality, since mitochondria in eggs fuel early embryonic development. Research suggests doses between 200 and 600 mg per day, and many specialists prefer the ubiquinol form for women over 35 because it's more readily absorbed. It won't reverse age-related declines entirely, but it's one of the most consistently cited options for women with diminished ovarian reserve or those preparing for IVF.

Low vitamin D levels have been associated with irregular ovulation, polycystic ovary syndrome (PCOS), and lower IVF success rates. A simple blood test can reveal your current level. Most fertility specialists prefer to see levels between 40 and 60 ng/mL. If you're deficient, 2,000 to 4,000 IU of D3 daily is a common starting point — though the exact dose should be guided by your bloodwork. Vitamin D3 paired with K2 improves calcium metabolism and may enhance overall hormonal regulation, making this combination worth asking your doctor about.
Expecting a supplement to compensate for chronic stress, poor sleep, or an unbalanced diet isn't realistic. A sustainable fertility plan treats supplementation as one pillar among several, not the entire structure. That means combining targeted nutrients with lifestyle habits — including regular movement — that support hormonal health across months, not days. The supplements you choose work best when the rest of your daily routine isn't actively working against them.
Most fertility-focused nutrients need time to accumulate before they have a measurable impact. CoQ10 can take 8 to 12 weeks to significantly raise levels in follicular fluid. Folate needs to be present before the neural tube begins forming. Vitamin D levels shift slowly. Starting your regimen at least three months before you plan to conceive gives the key supplements time to work. Regular physical activity supports this foundation too. If you're looking for low-impact cardio that's easy to maintain alongside a supplement routine, stair steppers offer a solid option that many women find sustainable without overtaxing their joints.
Some practitioners recommend adjusting your supplement protocol based on your menstrual cycle phase. Vitamin B6, which supports progesterone production, may be more useful in the luteal phase after ovulation. Antioxidants like CoQ10 and vitamin E are relevant throughout, but particularly during follicular development. This level of customization isn't necessary for everyone. But if you've been on a broad prenatal for several months without improvement, a phase-specific approach is worth discussing with a reproductive endocrinologist. It shifts the question from "what should I take" to "when and how much" — which is often where the real answer lies.
Consistency separates real results from wasted money. Taking a fertility supplement a few days a week and skipping the rest is functionally similar to not taking it at all for nutrients that require sustained blood levels. Building the daily habit is as important as choosing the right product — maybe more so, because the best formula does nothing sitting in a cabinet.
Oil-based supplements — CoQ10, omega-3 fatty acids, vitamin D — degrade faster when exposed to heat, light, or humidity. Store them in a cool, dry location away from the bathroom cabinet, where steam from showers can compromise capsule integrity over time. Probiotics, if your prenatal includes them, usually require refrigeration — check the label. Don't buy in bulk unless you cycle through supplements quickly. Check the expiration date on a new bottle before you start it, and discard anything that smells off or has changed in color or texture.
Combining a prenatal with individual supplements makes it easy to lose track of what you're actually ingesting. A simple note on your phone — or a dedicated app — keeps things clear and helps you spot unintentional double-dosing. It also gives your doctor an accurate picture if they ask you to disclose your full supplement routine. Hormonal shifts during a new regimen can affect more than just your cycle. Some women notice skin changes as their body adjusts. If that happens, looking into dermatologist-recommended acne products can help you manage any breakouts without disrupting your supplement schedule.
Take your supplements at the same time each day — pairing fat-soluble nutrients like vitamin D and CoQ10 with a meal that contains healthy fat significantly improves how much your body actually absorbs.
Even a well-chosen supplement can underperform if you're taking it under conditions that limit absorption. Small timing adjustments and a few basic rules around what to avoid can make a meaningful difference in how well your body uses what you're giving it. These aren't complicated changes — they're just details most people don't think about until something isn't working.
Fat-soluble vitamins — D, E, K, and A — require dietary fat to be absorbed efficiently. Take these with a meal that includes healthy fats like avocado, olive oil, eggs, or nuts. Water-soluble vitamins like folate and vitamin C can be taken any time, though many women find B vitamins sit better on a full stomach. If your prenatal contains iron, taking it with vitamin C boosts absorption. Taking it on an empty stomach maximizes uptake but can cause nausea in some women — with food is a reasonable trade-off if nausea is a problem for you.
Calcium and iron compete for absorption, so if your prenatal includes both, splitting them into morning and evening doses is a simple fix. Alcohol reduces the bioavailability of folate and B vitamins, which is one more reason to cut back during the preconception window. Some herbal supplements marketed for fertility — vitex, maca, black cohosh — can interact with hormonal medications or have effects that aren't well-studied. Always tell your doctor about every supplement you're taking, not just the prescription ones. That includes anything labeled "herbal," "natural," or "traditional."
The supplement industry operates with far less regulatory oversight than pharmaceuticals. That means marketing claims can outpace the actual science. Evaluating a product before you buy requires looking past the front label to the details that actually matter — and knowing what a red flag looks like when you see one.

Look for the active, bioavailable form of each ingredient. "Folic acid" is not equivalent to "methylfolate" for women with MTHFR variants. "Magnesium oxide" has poor absorption compared to magnesium glycinate or citrate. The label should specify the form, not just the nutrient name. Also scan the "other ingredients" section for fillers, artificial dyes, or allergens you want to avoid. Proprietary blends that don't disclose individual ingredient amounts — lumping everything under one undisclosed total — are generally a sign to look elsewhere. You deserve to know exactly what you're putting in your body.
Certifications from USP, NSF International, or Informed Sport mean an independent lab has verified that the product contains what the label claims and isn't contaminated with heavy metals or undisclosed substances. This matters more for fertility supplements than for everyday vitamins — you're likely taking these for months, potentially during early pregnancy. Spending a few extra dollars on a third-party verified product is a defensible trade-off when reproductive health is on the line. Look for the certification seal directly on the label, not just a claim on a website.
The fertility supplement market runs on hope, and hope is easily exploited. Some of the most widely repeated beliefs about supplements are either unsupported by evidence or actively misleading. Here's what deserves more skepticism — and why the conventional wisdom around fertility supplementation is sometimes wrong.

Higher doses don't reliably produce better outcomes — and in some cases, they create new problems. Vitamin A in excess is teratogenic, meaning it can cause birth defects, which is exactly why prenatal formulas use beta-carotene instead. Zinc in large amounts depletes copper. Even folate in very high doses can mask B12 deficiency, allowing a separate problem to go undetected. Staying within established recommended ranges isn't being conservative; it's being safe. If you think you need doses above what's found in standard prenatal formulas, work with your doctor rather than self-prescribing based on internet research.
Megadosing is not a strategy — for several key fertility nutrients, excessive intake can interfere with other nutrients or cause harm during early pregnancy.
No prenatal formula replicates what whole foods deliver. A supplement gives you isolated nutrients; leafy greens give you folate plus fiber, antioxidants, and phytonutrients that work together in ways researchers are still mapping. Supplements fill specific gaps — they don't substitute for meals. If your daily diet is built primarily around processed food, improving the diet is the priority, and supplements address what's still missing after that. Nutrient delivery also depends on your circulation. If that's a concern, understanding how to address poor circulation is worth your attention alongside any supplement protocol, since nutrients can only help if they're reaching the right tissues.
If you've been consistent with a fertility supplement regimen for three to six months and your situation hasn't changed, it's time to look deeper. Supplements can address nutritional gaps — they can't override structural or hormonal issues that require medical evaluation. Staying in a supplement loop without asking harder questions is a common way to delay treatment that might actually help.
PCOS, hypothyroidism, elevated prolactin, endometriosis, and uterine fibroids can all make conception difficult regardless of your supplement stack. If you haven't had a full hormonal panel, a thyroid function test, and an AMH (anti-Müllerian hormone) test, that's where the conversation with your doctor should begin. A reproductive endocrinologist can interpret these results in the context of your specific fertility picture. Supplements are an adjunct to medical care — not a diagnostic tool and not a substitute for one.
Sometimes the issue isn't which supplement you're taking — it's the form. Women with the MTHFR variant who've been taking standard folic acid may respond better to methylfolate. Women over 35 on ubiquinone CoQ10 may benefit from switching to ubiquinol. The product that works for someone else may not work for you for genetic and metabolic reasons. A functional medicine practitioner or integrative OB-GYN can help you figure out whether a form or dose change is worth exploring based on actual lab work rather than trial and error.
Not every fertility supplement is appropriate at every stage of your journey. Some are best used preconception; others can continue safely into pregnancy, while a few should be discontinued once you have a positive test. Knowing the difference can protect both you and any future pregnancy — and it's a conversation worth having with your provider before you start, not after.
Ideally, begin a fertility-focused supplement routine three to six months before you plan to start trying. This gives folate time to establish adequate red blood cell levels, CoQ10 time to accumulate in follicular fluid, and vitamin D time to reach an optimal range. If you've recently stopped hormonal contraceptives, allowing your body a couple of months to re-establish natural hormonal rhythms before adding supplements can simplify the picture. If you've been trying for six months without success — or three months if you're over 35 — talk to a doctor before expanding your stack, since some supplements may interact with fertility medications.
Once you have a confirmed positive pregnancy test, transition to a prenatal formulated specifically for pregnancy. Your preconception supplement stack may not be appropriate for a developing fetus. Vitex and maca, both popular for cycle support, haven't been studied in pregnancy and are generally not recommended. High-dose CoQ10 supplementation also lacks adequate safety data during pregnancy. When in doubt, consult your OB before continuing any supplement you started preconception. The goal at that point shifts entirely to supporting a healthy pregnancy, not maximizing conception odds.
Choosing between so many options can feel overwhelming. This table gives you a side-by-side look at the most commonly recommended of the best fertility supplements for women, what each one targets, typical dosing, and the strength of the evidence behind it. Use it as a starting framework, not a final prescription.
| Supplement | Primary Benefit | Typical Daily Dose | Evidence Level | Best Suited For |
|---|---|---|---|---|
| Methylfolate / Folic Acid | Neural tube protection, hormonal support | 400–800 mcg | Strong | All women preconception |
| CoQ10 (Ubiquinol) | Egg quality, mitochondrial energy | 200–600 mg | Moderate–Strong | Women over 30 or with diminished ovarian reserve |
| Vitamin D3 | Ovulation regularity, implantation | 2,000–4,000 IU | Moderate | Women with deficiency or PCOS |
| Myo-Inositol | Insulin sensitivity, ovulation support | 2,000–4,000 mg | Moderate | Women with PCOS |
| Omega-3 (DHA/EPA) | Inflammation reduction, embryo support | 1,000–2,000 mg | Moderate | Low fish intake, systemic inflammation |
| Iron | Ovulatory function, blood support | Per lab results | Moderate | Women with iron-deficiency anemia |
| Vitamin B6 | Luteal phase support, progesterone balance | 10–25 mg | Moderate | Short luteal phase |
| Zinc | Hormonal balance, egg maturation | 8–15 mg | Moderate | Women with irregular cycles |
This table is a starting point for a conversation with your healthcare provider — not a self-prescribing checklist. Your specific needs depend on your bloodwork, cycle history, age, and any diagnosed conditions. A high-quality prenatal may already cover several of these bases. Use the table to identify potential gaps, then verify whether those gaps actually exist with lab testing. Guessing at what you need without data is how women end up taking six supplements when one or two targeted choices would have been enough.



The best fertility supplement is the one you take consistently, chosen based on your actual nutritional gaps — not the one with the most impressive packaging.





About Prof. Raoul Orvieto
Professor Raoul Orvieto is a full professor of Obstetrics and Gynecology at the Sackler Faculty of Medicine, Tel-Aviv University, Israel, where he holds the Tarnesby-Tarnowski Chair for Family Planning and Fertility Regulation. He serves as director of the Division of Reproductive Endocrinology and Infertility at Sheba Medical Center (Tel-Hashomer), one of the largest medical centers in the Middle East. His research spans reproductive endocrinology, infertility treatment, and evidence-based fertility regulation.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below