
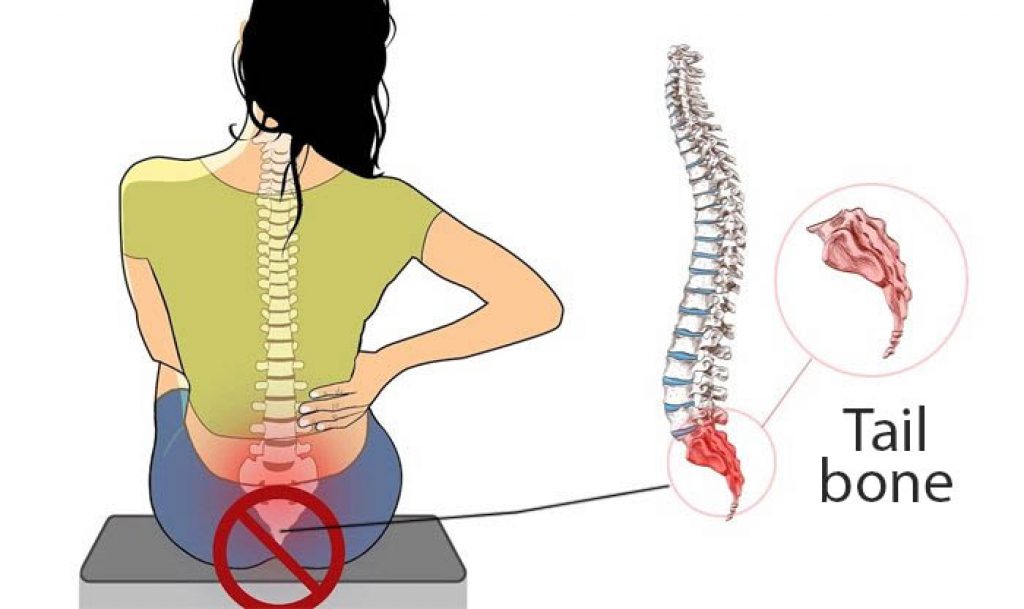
Tailbone pain when sitting and standing is a genuine medical condition — called coccydynia — and it responds well to targeted, non-surgical strategies once you understand what's driving it. The coccyx, the small triangular bone at the base of your spine, bears significant pressure during seated activities and during transitions between positions, which is why even ordinary daily movements can become sources of sharp, localized discomfort. Exploring your options through a broader look at joint and pain conditions can help you see how coccydynia fits into the wider picture of musculoskeletal health.
The condition affects women roughly five times more often than men, largely due to structural differences in the female pelvis and the strain of childbirth, though anyone who spends extended hours seated — at a desk, in a vehicle, or on a hard surface — can develop it over time. According to MedlinePlus, coccydynia encompasses causes ranging from acute injury to repetitive strain, and knowing which category applies to you shapes the most effective path forward.
The discomfort can range from a dull persistent ache to a stabbing sensation that radiates into the lower back or thighs, and many people find the transition between sitting and standing is the most painful moment of all, because the movement shifts the coccyx's angle dramatically. If you're also managing lower back pain, the two conditions often share overlapping causes and benefit from similar approaches.
Contents
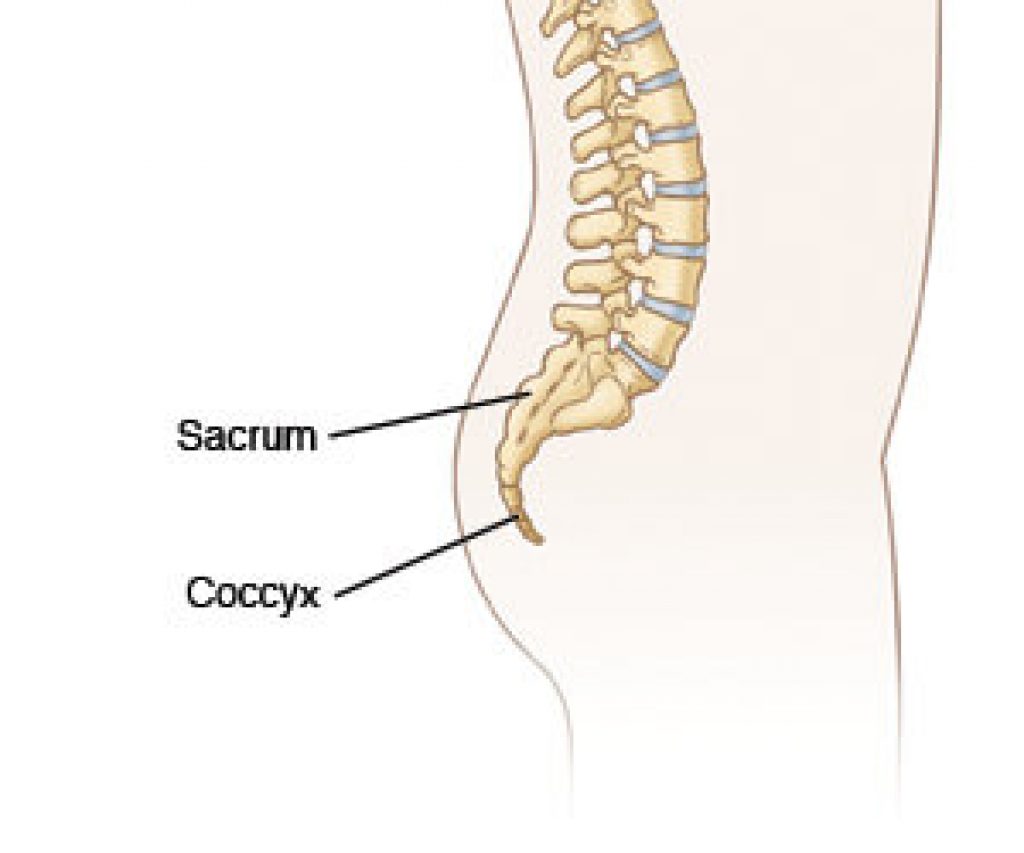
The coccyx is a surprisingly mobile structure made up of three to five fused vertebrae, and that mobility is precisely what makes it vulnerable to injury and chronic irritation. Coccydynia can stem from a single traumatic event or build gradually from repetitive stress, and identifying your specific cause matters when you're choosing a treatment strategy.

A fall onto a hard surface — a slip on ice, a tumble down stairs, or a hard landing during sport — is one of the most common triggers, and even a fall from months ago can leave residual inflammation or an undiagnosed fracture. Childbirth-related coccyx displacement is another significant cause, as the coccyx must flex to allow passage during delivery and sometimes doesn't return to its original position. Prolonged cycling on a narrow saddle and even long-distance driving can create enough repetitive micro-trauma to provoke coccydynia over time.
When you sit for extended periods on a firm or narrow chair without support, body weight that normally distributes across the sitting bones shifts backward onto the coccyx, loading a structure that wasn't designed to bear it directly. Slouching may feel comfortable in the short term, but it tilts the pelvis in a way that increases coccygeal pressure significantly, which is why many desk workers notice the pain intensifying progressively across a workday. Conditions like hemorrhoids can co-exist with coccydynia and occasionally create confusion about exactly where the pain originates.
Understanding what aggravates your coccyx is often just as valuable as knowing what helps it, because certain very common behaviors quietly sustain the problem day after day while you wonder why you're not improving.
Leaning back hard into a firm chair concentrates pressure directly on the coccyx and surrounding ligaments, while crossing your legs at the knee shifts weight asymmetrically and torques the pelvis in ways that persist even after you uncross. Sitting on a wallet or phone in your back pocket creates a pelvic tilt that loads one side of the coccyx more than the other, and this imbalance accumulates quietly throughout the day without obvious cause.
Rising straight up from a chair by pushing through your heels — rather than leaning forward first — forces the coccyx to bear more load as the pelvis pivots through the transition. Doing this dozens of times per day accumulates significant irritation. Bending forward from the waist rather than hinging at the hips during everyday tasks adds flexion stress to an already-sensitive area, and this movement pattern often becomes habitual without awareness.
Several widespread beliefs about coccydynia lead people to delay effective treatment or pursue approaches that don't match the evidence, and clearing them up can save you weeks of unnecessary suffering.
A common assumption is that complete bed rest will accelerate healing, but prolonged inactivity actually weakens the muscles that support the pelvis and spine, making it harder to offload pressure from the coccyx when you return to normal activity. Most clinical guidance favors staying gently active rather than immobilized, with light walking and targeted stretching proving more beneficial than extended rest for soft-tissue and joint conditions affecting the coccyx.
While mild coccydynia from minor overuse often improves within a few weeks without specific treatment, persistent pain lasting longer than a month rarely resolves on its own without active intervention. People who wait for spontaneous resolution can develop chronic patterns of muscle guarding and compensatory movement that make recovery significantly harder over time, and addressing the condition early tends to produce better long-term outcomes. If chronic pain is also disrupting your sleep, the strategies in this guide on sleeping better with persistent pain offer approaches that transfer well across pain conditions.
A layered approach to managing tailbone pain when sitting and standing gives you the best chance of lasting relief rather than just temporary symptom suppression, moving from immediate comfort measures toward longer-term rehabilitation.
Applying ice wrapped in cloth for fifteen to twenty minutes several times a day during acute flares reduces local inflammation effectively, and after the initial phase passes, switching to heat relaxes the surrounding muscle tension that often amplifies coccygeal pain. Over-the-counter NSAIDs like ibuprofen or naproxen address both inflammation and pain, though consistent daily use beyond a week or two warrants a conversation with your healthcare provider. Using a specialized coccyx cutout cushion whenever you sit is one of the fastest ways to reduce mechanical loading throughout the day without any other intervention.
Gentle pelvic floor relaxation exercises and deep hip stretches — particularly the piriformis stretch performed lying on your back — reduce muscular tension that compresses the coccygeal region, and doing these consistently over several weeks produces cumulative benefit. Strengthening your glutes and core provides a muscular buffer that keeps pressure off the coccyx during sit-to-stand transitions, and tools like the Chirp Wheel can help mobilize the surrounding spinal segments to reduce referred tension. Low-impact cardiovascular work on a recumbent exercise bike keeps you fit and promotes circulation without placing direct pressure on the tailbone.
Most people respond well to conservative measures, but understanding the full spectrum of available options helps you make informed decisions about how aggressively to pursue treatment and at what point to involve a specialist.
| Treatment Option | How It Works | Advantages | Limitations |
|---|---|---|---|
| Coccyx cushion | Redistributes pressure away from the tailbone | Immediate relief, affordable, no side effects | Doesn't address the underlying cause |
| NSAIDs | Reduces systemic inflammation and pain | Fast-acting, widely available | GI side effects with prolonged use |
| Physical therapy | Strengthens support muscles, improves movement mechanics | Addresses root cause, durable results | Requires consistent commitment over weeks |
| Corticosteroid injection | Reduces localized inflammation directly at the coccyx | Can provide weeks to months of relief | Invasive, temporary, limited repeat doses |
| Massage therapy | Releases tension in pelvic floor and gluteal muscles | Non-invasive, improves tissue mobility | Results vary, may require ongoing sessions |
| Coccygectomy (surgery) | Surgical removal of the coccyx | Permanent resolution for refractory cases | Significant recovery period, reserved for severe cases |

A quality coccyx cushion is arguably the single most impactful daily-use tool for managing tailbone pain when sitting and standing, because it removes the primary mechanical stressor during the activity that causes the most discomfort, and the options vary significantly in material, cutout depth, and portability.
The ComfiLife Gel Enhanced Seat Cushion uses a gel-infused memory foam layer that conforms to your contours while the coccyx cutout suspends the tailbone completely above the surface.

The Aylio Coccyx Orthopedic Comfort Foam Cushion is a flatter, lightweight option that travels well between multiple seating environments and works reliably on most standard chair types.

For people who need firmer support with a deeper cutout, the LoveHome Memory Foam Seat Cushion (B01MZ8IVP4) offers a structured base that holds its shape through full workdays without compressing flat.

The Everlasting Comfort Seat Cushion features a wide U-shaped cutout and a non-slip cover, making it a popular choice for extended desk sessions and long commutes where the coccyx needs sustained unloading over several hours.

If your mobility is significantly affected and transitioning between positions has become difficult and painful, reviewing what's available in terms of mobility aids and how they improve daily function may introduce options worth discussing with your care team.
If your tailbone pain has lasted more than six to eight weeks despite consistent conservative care, or if you're experiencing numbness, radiating leg pain, or bladder and bowel changes, seeing a healthcare provider is the appropriate next step rather than continued self-management. A physician may recommend imaging to rule out fractures or referred pain from other sources, and a referral to a pelvic floor physical therapist can provide manual therapy with a strong evidence base for coccydynia. It's also worth noting that people who alter their gait to avoid tailbone pain sometimes develop secondary issues — conditions like heel pain can emerge when compensatory movement patterns place new stress on structures further down the kinetic chain.
The medical term is coccydynia, which refers to pain localized to the coccyx — the small triangular bone at the base of the spine — that typically worsens with sitting, rising from a seated position, or direct pressure on the area.
Mild cases often improve within a few weeks with conservative management, while more persistent cases can take several months of active treatment, and a small percentage of people develop chronic coccydynia that requires medical intervention beyond home care.
Prolonged sitting alone is unlikely to cause permanent structural damage in most people, but it can perpetuate inflammation and chronically irritate the coccygeal ligaments, making recovery slower if the underlying pressure source isn't addressed.
Yes, walking is generally beneficial because it promotes circulation, keeps pelvic muscles active, and avoids the direct compressive loading that sitting creates — though maintaining good posture and avoiding jarring terrain matters during the recovery period.
A poorly fitted or excessively soft cushion can allow the tailbone to sink through and still contact the firm base below, providing little real relief, so choosing one with a firm enough foundation and a clearly defined cutout that keeps the coccyx fully suspended is important.
High-impact activities like running on hard surfaces, cycling on narrow saddles, rowing, and any exercise involving direct seated pressure on the coccyx are best modified or avoided until your symptoms are sufficiently under control to tolerate them without aggravation.
The two conditions are distinct but can co-exist; sciatica involves the sciatic nerve and typically produces radiating leg pain, while coccydynia is localized to the tailbone, though both can arise from pelvic instability or structural changes in the lower spine.
In most cases it reflects a benign musculoskeletal issue, but tailbone pain with no clear cause, unexplained weight loss, or no response to conservative treatment warrants medical evaluation to rule out less common causes like tumors or referred pain from pelvic organ conditions.





About Dr. Marshall Emig, MD
Dr. Marshall Emig is a physiatrist and associate professor at the University of Colorado School of Medicine, practicing at UCHealth in Colorado. He holds board certifications in physical medicine and rehabilitation, sports medicine, and neuromuscular medicine, and has over twenty years of clinical experience. His practice focuses on musculoskeletal conditions including arthritis, spinal stenosis, carpal tunnel syndrome, and chronic pain management.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below