
A heel spur is a bony calcium deposit that builds up on the underside of the heel bone over months or years of repetitive strain. Understanding heel spur causes and treatment is the fastest route to real relief — and here's the good news: the vast majority of cases resolve without surgery. This guide covers causes, symptoms, treatment tiers, and when to seek professional help. For more foot health resources, visit RipPain's foot care section.
Heel spurs are closely linked to plantar fasciitis — the inflammation of the thick fibrous band running along the bottom of the foot. Studies suggest that around 70% of people diagnosed with plantar fasciitis also have a detectable heel spur on imaging. Yet the spur itself is often not the direct pain source. It's the inflamed surrounding tissue that triggers that sharp, stabbing morning sensation.
Many people carry heel spurs with zero symptoms. For those who do feel them, discomfort ranges from a mild post-activity ache to severe pain that limits every step. Either way, identifying what's happening inside that heel — and matching it to the right response — changes the trajectory completely.
Contents
Misinformation about heel spurs is everywhere, and it leads people toward unnecessary fear — or unnecessary ignoring of a fixable problem. Let's reset the record on the most persistent misconceptions.
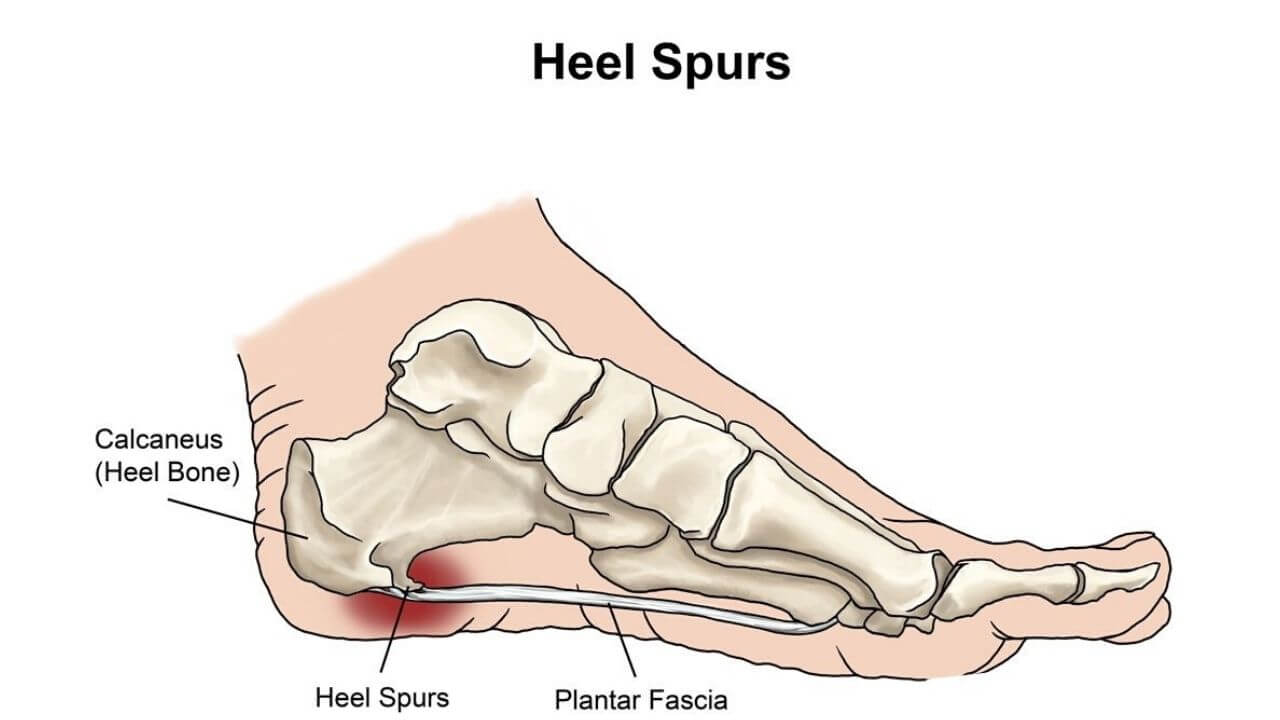
Most people assume the bony growth itself is the source of pain. That's rarely accurate. A heel spur is not a jagged spike — it's a smooth bony outgrowth that forms gradually in response to repeated pulling of the plantar fascia and surrounding soft tissues on the heel bone.
Pro insight: Treating the spur without addressing the underlying strain pattern — poor footwear, tight calves, excess body weight — almost always leads to symptom recurrence.
These two conditions overlap heavily but they are not the same thing. Plantar fasciitis is an inflammatory soft tissue condition; a heel spur is a structural bony formation. One can exist without the other, though they frequently co-occur.
| Feature | Plantar Fasciitis | Heel Spur |
|---|---|---|
| Nature | Soft tissue inflammation | Bony calcium deposit |
| Diagnosis method | Physical exam + symptoms | X-ray confirmation |
| Always painful? | Yes, during the active phase | No — often asymptomatic |
| Primary treatment | Stretching, orthotics, rest | Same as plantar fasciitis |
| Surgical rate | ~5–10% of cases | Rare — only when conservative care fails completely |
Early intervention transforms outcomes. The gap between a mild heel spur case and a chronic, debilitating one often comes down to how quickly and consistently treatment begins.
Early heel spur pain has recognizable hallmarks that distinguish it from other foot conditions:
At this stage, consistent stretching and footwear adjustments resolve most cases within 6–8 weeks.
Ignored early symptoms harden into chronic patterns. When pain persists beyond three months despite basic self-care, the condition is classified as chronic. At that point:
Chronic cases require structured intervention — physical therapy, custom orthotics, or medical procedures — rather than stretching alone.
For both prevention and active recovery, daily habits carry more therapeutic weight than any single intervention. Consistency matters far more than intensity.
The goal is to reduce tension on the plantar fascia and Achilles tendon, which directly offloads stress from the heel bone. These five moves form a reliable daily protocol:
Tip: Doing the plantar fascia stretch before the very first step of the morning dramatically reduces that notorious stabbing pain — it's one of the most consistently validated self-care moves for this condition.
Shoes are arguably the single most impactful daily variable in heel spur management. The right features make a measurable difference:
Pairing supportive footwear with compression socks adds another layer of arch support and helps reduce post-activity swelling — a combination that makes a noticeable difference in day-to-day comfort for chronic sufferers.
Heel spur causes and treatment aren't one-size-fits-all. Contributing factors and best interventions shift considerably depending on a person's activity level, occupation, and body composition.
Runners, basketball players, and people who spend hours on hard floors carry elevated risk. The most common contributing factors include:
Athletes benefit significantly from plantar fasciitis walking boots during acute flare-ups — they immobilize the foot to let inflammation settle while keeping the person mobile. Understanding how a plantar fasciitis boot works and when to use one helps athletes decide when to rest the structure completely versus when to modify training and push through carefully.
Heel spurs aren't exclusive to active populations. Prolonged sitting followed by sudden standing, combined with excess body weight, creates its own distinct strain pattern:
Weight management is a core pillar of long-term heel spur relief for this group. Even a modest reduction in body weight produces measurable decreases in plantar pressure during normal walking.
A solid long-term strategy layers conservative self-care with escalating medical options when needed. Most people never move beyond the first two tiers.
When stretching and footwear changes don't resolve pain within 6–8 weeks, these evidence-based options are the appropriate next step:
Surgery is reserved for cases that fail to improve after 9–12 months of comprehensive conservative care. The options are narrow and specific:
Knowing when to escalate care prevents both under-treatment and over-medicalization. The decision comes down to a handful of clear signals.
Seek professional evaluation when any of the following apply:
Conservative home management is appropriate — and frequently fully effective — when:
In these scenarios, the daily stretching protocol, the right shoes, proper foot care tools to keep skin and tissue healthy, and reduced high-impact activity resolve the problem in the majority of cases within 2–3 months. Patience and consistency do more work here than any single product or intervention.
A heel spur is a bony calcium deposit that forms on the underside of the calcaneus (heel bone). It develops gradually in response to repeated mechanical stress — usually from tight plantar fascia or Achilles tendon pulling repeatedly on the heel bone over months or years.
No, though they frequently co-exist. Plantar fasciitis is an inflammatory condition of the fibrous band along the foot's arch. A heel spur is a structural bony formation. About 70% of plantar fasciitis patients also have a heel spur, but the two conditions are diagnosed and can occur independently.
Heel spurs form from repetitive strain on the heel bone. Common causes include long hours standing or walking on hard floors, running without proper footwear, excess body weight, flat feet or high arches, tight calf muscles, and wearing shoes that lack adequate arch support or cushioning.
Most cases improve significantly within 6–8 weeks of consistent conservative care — daily stretching, supportive footwear, and activity modification. Chronic cases may take 6–12 months. Less than 10% of people ultimately require medical procedures beyond basic conservative management.
The bony spur itself rarely disappears — bone deposits are typically permanent. However, the pain associated with heel spurs resolves completely in the vast majority of cases through conservative treatment. Asymptomatic spurs discovered incidentally on imaging require no treatment at all.
The best footwear for heel spurs features a deep heel cup, firm midsole, adequate arch support, and a modest heel raise (not completely flat). Motion-control or stability running shoes work well for everyday use. Custom orthotics from a podiatrist provide the most targeted fit for persistent cases.
Surgery is considered only after 9–12 months of comprehensive conservative treatment — including physical therapy, orthotics, and at least one medical procedure like ESWT or corticosteroid injection — has failed to produce meaningful improvement. Fewer than 5% of heel spur cases reach this threshold.
The heel spur itself is rarely the real enemy — the habits, footwear, and imbalances that created it are, and fixing those is what actually brings lasting relief.





About Mehnaz
Mehnaz is the founder and editor of RipPain, a health resource site dedicated to helping readers navigate pain management, recovery, and medical device research. Her work on the site is driven by personal experience caring for seriously ill family members, which led her to study evidence-based guidance from physicians, pain specialists, and published medical research. She curates and summarizes expert medical insights to make credible health information accessible to everyday readers.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below