
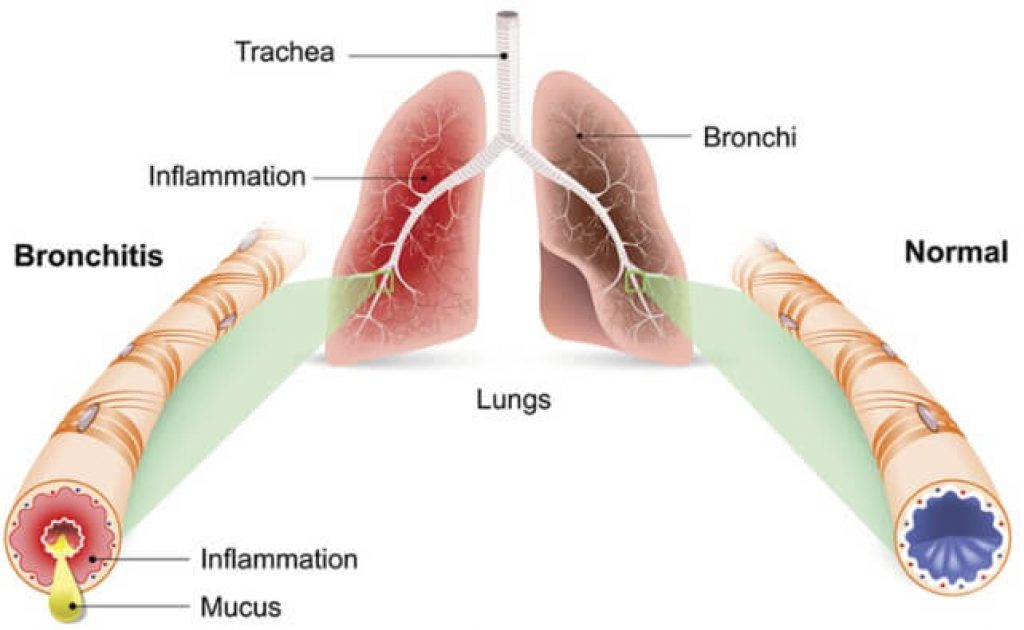
Knowing how to treat bronchitis effectively starts with one clear truth: acute bronchitis is almost always viral, which means antibiotics do nothing for it. Your treatment strategy centers on symptom management, airway support, and letting your immune system resolve the infection on its own timeline. Bronchitis inflames the bronchial tube lining, triggering mucus overproduction and that signature deep cough — and your approach in the first 48 hours determines whether you recover in a week or drag through three.
The bronchial tubes, when inflamed, produce excess mucus as a protective response. That cough you're fighting is your airways working exactly as designed — mobilizing secretions, clearing debris, pushing pathogens out. Understanding this mechanism changes everything about how you approach treatment. You're not fighting the cough. You're supporting the process. The irritation, fatigue, and chest tightness all have a physiological basis that responds to specific, targeted interventions when you apply them correctly.
This guide walks you through the clinical picture, the evidence-based treatment protocol, and the monitoring tools that genuinely accelerate recovery. Whether you're managing your first acute episode or a recurrent pattern, the approach here is grounded in what the evidence actually shows — not what gets prescribed reflexively.
Contents
Bronchitis is inflammation of the bronchial tube lining — the airways that carry air from your trachea into your lung tissue. When a viral pathogen takes hold in this tissue (most commonly rhinovirus, influenza, or RSV), the mucosal lining swells and begins secreting excess mucus as both a barrier and a pathogen trap. The result is narrowed airways, impaired mucociliary clearance, and a cough that can feel relentless even when it's doing exactly what it should.
According to the CDC, acute bronchitis accounts for millions of outpatient visits annually, and the vast majority of cases resolve without pharmaceutical intervention. What separates a fast recovery from a prolonged one is how intelligently you support your body's natural resolution process — not whether you get a prescription.

Acute bronchitis runs its course in 10–20 days for most people. The cough alone can persist up to 3 weeks post-infection — that's normal bronchial healing, not treatment failure. Chronic bronchitis, by contrast, is defined clinically as a productive cough lasting at least 3 months in each of two consecutive years, and it falls squarely under the COPD umbrella. These two conditions require fundamentally different management strategies, and conflating them leads to poor decisions in both directions.
If you smoke or have significant occupational exposure to dust, chemicals, or airborne irritants, you're facing a different clinical picture than a healthy adult who picked up a winter respiratory virus. Recognizing which category applies to you determines whether you're managing an episode or managing a lifelong condition.
Viral infection drives over 90% of acute bronchitis cases. Bacterial causes — Mycoplasma pneumoniae, Chlamydia pneumoniae, Bordetella pertussis — account for fewer than 10%, which explains precisely why blanket antibiotic prescribing produces harm rather than benefit. Beyond infectious triggers, airway irritants including cigarette smoke, air pollution, chemical fumes, and chronic GERD can trigger bronchitic inflammation without any pathogen involvement whatsoever. Understanding the trigger matters for prevention as much as treatment.
Bronchitis sits at the center of some remarkably persistent clinical myths — myths that drive poor treatment decisions, delay recovery, and fuel antibiotic resistance at a population level. Clearing these up is not academic; it changes what you do from day one.
The most damaging myth in bronchitis management is that antibiotics accelerate recovery. Multiple randomized controlled trials have found no clinically meaningful benefit from antibiotics in acute bronchitis in otherwise healthy adults. Yellow or green mucus does not signal bacterial infection — it signals neutrophil activity, which occurs in viral infection just as readily as in bacterial. Demanding antibiotics for bronchitis is one of the primary drivers of antibiotic-resistant organisms, and it does not shorten your illness by a single day.
Clinical guidelines from both the American Academy of Family Physicians and the American College of Chest Physicians align unambiguously: routine antibiotics for acute bronchitis are not recommended. The presence of purulent sputum has no meaningful predictive value for bacterial versus viral etiology. This is settled medicine, not a matter of clinical debate.
The other persistent myth is that complete bed rest is the optimal response. Prolonged immobility during respiratory illness impairs mucociliary clearance, reduces pulmonary function, and compounds the circulatory effects of reduced activity. Light, controlled movement — short walks, gentle breathing exercises — maintains lymphatic circulation and actively supports immune function. Those dealing with prolonged sedentary recovery periods should review guidance on what to do about poor circulation, since respiratory illness and immobility compound circulatory stress significantly in vulnerable individuals.
Never suppress a productive cough entirely — your airways depend on it to clear secretions. Reserve cough suppressants for nighttime only, when coughing genuinely disrupts sleep.
Learning how to treat bronchitis effectively means executing the right interventions in the right sequence, not reaching for whatever is closest in the medicine cabinet. Here is the clinical protocol that holds up under scrutiny.
In the acute phase, your three goals are hydration, airway moisture, and fever management. Consume a minimum of 2–3 liters of fluid daily — warm liquids (herbal teas, bone broth, warm water with honey) thin mucus more effectively than cold water and deliver a secondary soothing effect via gentle steam. Honey, specifically raw honey at 1–2 tablespoons, has demonstrated genuine antitussive and antimicrobial properties in peer-reviewed trials. It is not folk medicine. It is evidence-based practice.
Humidification is non-negotiable. Dry air thickens bronchial secretions and prolongs the cough phase. A cool-mist humidifier in your sleeping space, set to 40–50% relative humidity, measurably reduces nighttime cough frequency. Steam inhalation — 10–15 minutes twice daily — achieves the same mucolytic effect acutely. Adding eucalyptus oil is supported by the documented bronchodilatory and anti-inflammatory properties of 1,8-cineole, its primary active compound.
Fever up to 101°F (38.3°C) is immunologically beneficial — do not reflexively suppress it. Above that threshold, acetaminophen or ibuprofen at appropriate therapeutic doses is warranted. Ibuprofen additionally addresses the inflammatory component of bronchial wall irritation directly, giving it a marginal advantage over acetaminophen alone in symptomatic management.
By day 3, acute viral replication is winding down, but airway inflammation persists. This is the window where most people err by returning to full activity too early. Continue hydration and humidification. Introduce diaphragmatic breathing exercises — five minutes every two to three hours actively recruits lower lobe ventilation and prevents atelectasis in the smaller airways.
Postural drainage is a technique respiratory therapists use routinely that you can apply at home. Lie with your hips elevated above your chest for 15–20 minutes to use gravity to mobilize secretions toward the larger central airways. Follow with controlled coughing: two controlled, deliberate coughs rather than one violent burst produces better secretion clearance without further damaging already-inflamed mucosa. This is the technique that actually moves mucus rather than just irritating the airway.
Nutritional emphasis in this phase should center on anti-inflammatory foods: omega-3-rich fish, leafy greens, garlic, ginger, and turmeric. An anti-inflammatory dietary approach is not exclusive to bronchitis — the same principles that apply to managing inflammatory conditions like gout (covered in depth in our guide on foods that help get rid of gout) translate directly to any condition driven by systemic inflammation, including bronchitic airways.
Effective bronchitis management is not passive. Tracking your respiratory status and deploying the right supportive tools turns treatment from guesswork into a measurable, adjustable process with clear decision points.
A pulse oximeter belongs in every home medicine cabinet. During bronchitis, SpO2 (peripheral oxygen saturation) can dip — particularly during sleep or light exertion — well before you subjectively feel impaired. A healthy baseline runs 95–100%. Readings consistently below 92% at rest require same-day medical evaluation. Tracking your daily readings gives you objective data on whether your airways are genuinely improving or quietly deteriorating.
A quality pulse oximeter is a modest investment with outsized diagnostic value. The 7 best pulse oximeters for home use include options accurate enough for clinical-grade monitoring without the clinical price tag. Pair oximetry readings with respiratory rate tracking — count breaths per minute for a full 60 seconds — for a complete picture of your respiratory status at each checkpoint.
| SpO2 Reading | Clinical Interpretation | Recommended Action |
|---|---|---|
| 95–100% | Normal range | Continue home management protocol |
| 92–94% | Mild hypoxemia | Increase rest and humidification; monitor every 2 hours |
| 88–91% | Moderate hypoxemia | Contact physician same day without delay |
| Below 88% | Severe hypoxemia | Emergency evaluation — call emergency services immediately |

N-acetylcysteine (NAC) is the most clinically supported mucolytic supplement available over the counter. It directly cleaves mucus disulfide bonds, reducing sputum viscosity and improving mechanical clearance. Doses of 600 mg twice daily have demonstrated efficacy across multiple trials for both acute bronchitis and COPD exacerbations. Pelargonium sidoides — the EPs 7630 extract derived from an African geranium — has solid randomized controlled trial evidence for reducing both the duration and severity of acute bronchitis, cutting sick days by approximately two days versus placebo. That is a clinically meaningful result.
Zinc lozenges — not oral supplements, but lozenges specifically for direct mucosal contact — show consistent benefit when used within the first 24–48 hours of symptom onset. Vitamin D deficiency correlates strongly with increased susceptibility and severity of respiratory infections; supplementation through deficiency is not optional in high-risk periods. Elderberry extract carries modest but reproducible immune-modulating effects in the acute phase and is worth including in your first-line supportive stack.
Both pharmaceutical and natural interventions have a place in bronchitis management. The mistake is over-relying on either. Understanding the actual trade-off profile of each approach lets you use them strategically rather than reflexively.
Bronchodilators — specifically albuterol via metered-dose inhaler — are indicated when audible wheezing is present or when spirometric testing confirms airflow obstruction. They work for bronchospasm. They do not work for infection. If you have concurrent asthma or reactive airway disease, your clinician will prescribe accordingly. Oral or inhaled corticosteroids reduce airway inflammation meaningfully in severe acute cases and in patients with underlying atopy. Neither drug class addresses the viral cause — they manage the inflammatory response so your airways can function while healing occurs.
Guaifenesin (expectorant) has mechanistic plausibility as a mucolytic and is appropriate OTC use despite mixed clinical trial results. Dextromethorphan for nighttime cough suppression has evidence-based support specifically for sleep-disrupting cough. Codeine-based suppressants are not first-line for acute bronchitis — addiction risk and side-effect burden are not justified by incremental benefit over OTC options in an otherwise healthy adult.
The natural approach is not a consolation prize — it is frequently the appropriate primary strategy. Hot showers leveraging steam inhalation, saline nasal irrigation (HyperSaline spray or neti pot technique), garlic supplementation for its well-documented allicin-mediated antimicrobial and anti-inflammatory properties, and ginger tea with raw honey constitute a regimen that simultaneously addresses inflammation, mucus viscosity, and immune function. The overlap between these mechanisms is additive.
For patients managing chronic bronchitis who want to maintain cardiovascular conditioning without exacerbating symptoms, the best rowing machine under $300 offers an excellent low-impact full-body option that can be dialed to minimal resistance during active recovery phases. Structured cardiovascular fitness genuinely improves pulmonary function and exercise tolerance over time in COPD and chronic bronchitis — the evidence base here is robust.
During extended recovery or chronic management periods when significant time is spent off your feet, venous return and peripheral circulation can compound systemic burden. Both graduated compression socks and proactive attention to overall vascular health — particularly for older adults or those with comorbid circulatory conditions — become relevant ancillary considerations. Our coverage on improving circulation in your feet and ankles covers practical daily strategies applicable during prolonged recovery phases.
A cough persisting beyond 3 weeks after acute bronchitis is not necessarily treatment failure. It often represents post-infectious airway hyperresponsiveness — a distinct clinical entity sometimes called post-bronchitic cough, where the airway remains sensitized and reactive after the infection has resolved. But it requires re-evaluation rather than continued self-management.
Certain clinical findings in a bronchitis presentation mandate prompt medical assessment without waiting to see if symptoms self-resolve:
Secondary bacterial pneumonia is the most serious complication of acute bronchitis, occurring when the damaged bronchial epithelium becomes susceptible to bacterial superinfection. This is one scenario where antibiotics are definitively indicated and urgently needed. The clinical picture of pneumonia — high sustained fever, consolidative cough, pleuritic chest pain, and significantly reduced SpO2 — is distinct from uncomplicated bronchitis and cannot be safely managed at home.
Chronic bronchitis management is a sustained, multifactorial effort with no shortcuts. Smoking cessation is the single most impactful intervention available — nothing else in the evidence base comes close for halting disease progression. Pulmonary rehabilitation, including structured breathing exercises, pacing strategies, and supervised graded exercise, improves quality of life and reduces exacerbation frequency with reproducible effect sizes. Annual influenza vaccination and pneumococcal vaccination meaningfully reduce the risk of acute-on-chronic exacerbations — two events that dramatically accelerate lung function decline.
Indoor air quality is chronically underestimated as a management variable. HEPA filtration in living spaces, avoidance of VOC-emitting products, and maintaining 40–50% relative humidity protect the bronchial mucosal environment between exacerbations. Chronic hypoxia from progressive disease also manifests beyond the respiratory tract — nail clubbing is a classic sign of long-term hypoxemia that patients frequently miss or misattribute. Learning to read the signs in your toenails and nails as systemic health markers is a practical skill for anyone navigating a chronic respiratory condition.
Nutritional management in chronic bronchitis parallels the acute anti-inflammatory approach but with greater emphasis on caloric adequacy. COPD and chronic bronchitis dramatically increase the energy cost of breathing, and malnutrition is a frequent and underdiagnosed complication that accelerates respiratory muscle wasting. High-protein, calorie-dense foods are the nutritional priority — not supplemental superfoods, but consistent macronutrient adequacy across every meal.
The acute infectious phase resolves within 7–10 days for most people, but the cough can persist for up to 3 weeks as your bronchial lining fully heals. A cough lasting beyond 3 weeks warrants medical evaluation to rule out post-infectious airway hyperresponsiveness, pertussis, or an underlying pulmonary condition that was unmasked by the acute episode.
Light activity — short walks, gentle stretching, diaphragmatic breathing exercises — is beneficial during recovery and supports mucociliary clearance. High-intensity exercise is contraindicated until you have been fever-free for 48 hours and your SpO2 holds consistently above 95% during exertion. If your respiratory rate climbs above 20 breaths per minute at rest, reduce activity further until the inflammation subsides.
Antibiotics are warranted only in specific circumstances: confirmed bacterial etiology via culture or rapid testing, clear clinical suspicion for pertussis, symptoms that improve and then acutely worsen suggesting bacterial superinfection, or significant underlying comorbidities that substantially elevate the risk of bacterial complications. In the otherwise healthy adult with typical acute bronchitis, antibiotics are not indicated and do not alter the clinical course by any meaningful measure.
You now have a complete framework for treating bronchitis effectively — from the acute 48-hour protocol through long-term chronic management. Start with the step-by-step protocol, add pulse oximetry to your recovery toolkit so you have objective data rather than subjective guesswork, and act immediately if any of the red flags outlined above appear. The sooner you apply the right interventions and stop relying on the wrong ones, the faster your airways recover — so take what you've read here and put it into practice today.





About Mehmet Kesimer, PhD
Mehmet Kesimer is an associate professor of pathology and laboratory medicine at the University of North Carolina at Chapel Hill, based at the Marsico Lung Institute. His research specializes in mucin biology and airway defense mechanisms, with a particular focus on how dysfunction in these systems contributes to chronic lung diseases including COPD, cystic fibrosis, and asthma. He collaborates closely with Dr. Richard C. Boucher and has published foundational research establishing mucin concentration as a diagnostic marker for chronic bronchitis and COPD progression.
You can get FREE Gifts. Or latest Free phones here.
Disable Ad block to reveal all the info. Once done, hit a button below